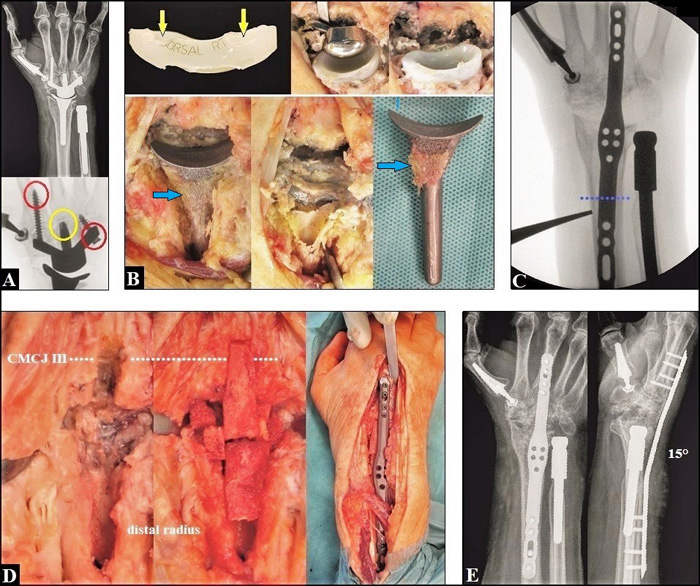
Fig. (7) Same patient as in Figs. (4 A-D and 6 A-E: (A) Eight years after TWA, there was evident loosening of carpal Maestro component with cortical migration of the radial-side non-locking screw distally, and loosening with the migration of the ulnar-side non-locking screw proximally into the articular space (red circles). Furthermore, as compared to Figs. (4 B-E), the carpal component is subsided (yellow circle). (B) Typically, the mechanical imbalance of carpal component led to polyethylene wear at the dorsal rim of the insert (yellow arrows), and metal wear originated from the holes of loosened capitate peg and screws, whereas the radial component was sufficiently osseointegrated (light blue arrows). A motion-preserving revision TWA with an exchange of carpal component was wished by the patient, but it was not possible due to the withdrawal of implant by the company. Thus, a TWF had to be performed. For removal of the non-cemented completely osseointegrated radial component, a large dorsal bony windowing at the distal radius became necessary. (C) Intraoperatively, planning the length of the 3,5/2,7 mm Acu-Loc wrist spanning plate (acumed, Hillsboro, Oregon/USA) bridging the large bony defect at the distal radius (pointed line). This plate has proven to be useful for TWF after a failed TWA [107]. (D) Intraoperative clinical photographs showing the sawed groove into the base of the 3rd metacarpal for placement of a corticocancelleous iliac crest bone graft crossing the 3rd carpometacarpal joint (CMCJ III, pointed line) after debridement of metal debris, and the low-profile 3,5 mm locking fusion plate after its insertion. (E) The TWF was done with the wrist in 15° extension and postoperative radiographs in both planes demonstrating correct placement of fusion plate bridging the large bony defect.