- Home
- About Journals
-
Information for Authors/ReviewersEditorial Policies
Publication Fee
Publication Cycle - Process Flowchart
Online Manuscript Submission and Tracking System
Publishing Ethics and Rectitude
Authorship
Author Benefits
Reviewer Guidelines
Guest Editor Guidelines
Peer Review Workflow
Quick Track Option
Copyediting Services
Bentham Open Membership
Bentham Open Advisory Board
Archiving Policies
Fabricating and Stating False Information
Post Publication Discussions and Corrections
Editorial Management
Advertise With Us
Funding Agencies
Rate List
Kudos
General FAQs
Special Fee Waivers and Discounts
- Contact
- Help
- About Us
- Search


The Open Anatomy Journal
(Discontinued)
ISSN: 1877-6094 ― Volume 6, 2014
Left Hepatic Artery Arising from the Superior Mesenteric Artery: A Case Study of a Rare Anatomic Variation
Eleazar Chaib*, Yngrid E.D.M de Souza, Marcelo Y Maruyama, Leonardo F.B Marinucci, Matheus R Aranha, Isabela A. de Siqueira, Lucas Chen, Mariana P.D de Campos Carvalho , Luiz A.C D’Albuquerque
Abstract
Knowledge of hepatic arterial vascularization and its variations have a significant relevance for the daily practice of hepato-biliary surgeon as well as radiologists. Human cadaver livers (n=60) were obtained from routine autopsies. Resections were carried out en bloc with liver, celiac trunk (CT), left gastric artery (LGA), lesser omentum, superior mesenteric artery (SMA) and head of the pancreas. We have found one case with an exceptional anatomic variation, replaced left hepatic artery (LHA) coming off the SMA directly to the hepatic left lobe. We would like to draw attention for this particularly anatomic variation of the origin of the LHA ensuring that no damage will be made during gastrointestinal surgery.
Article Information
Identifiers and Pagination:
Year: 2010Volume: 2
First Page: 76
Last Page: 78
Publisher Id: TOANATJ-2-76
DOI: 10.2174/1877609401002010076
Article History:
Received Date: 29/10/2009Revision Received Date: 6/11/2009
Acceptance Date: 15/3/2010
Electronic publication date: 14/5/2010
Collection year: 2010
open-access license: This is an open access article licensed under the terms of the Creative Commons Attribution Non-Commercial License (http: //creativecommons.org/licenses/by-nc/3.0/ which permits unrestricted, non-commercial use, distribution and reproduction in any medium, provided the work is properly cited.
* Address correspondence to this author at the Liver Transplantation Unit, and LIM 37, Hospital das Clinicas, Av. Dr. Enéas de Carvalho Aguiar 255, Level 9, CEP 05403-010, Sao Paulo, Brazil; Tel: 55-11-3061.8322; Fax: 55-11-30617270; E-mail: eleazarchaib@yahoo.co.uk
| Open Peer Review Details | |||
|---|---|---|---|
| Manuscript submitted on 29-10-2009 |
Original Manuscript | Left Hepatic Artery Arising from the Superior Mesenteric Artery: A Case Study of a Rare Anatomic Variation | |
INTRODUCTION
Knowledge of hepatic arterial vascularization and its variations have a significant relevance for the daily practice, basically the classic arterial anatomy is seen in 55 to 77% of the population [1, 2]. Anatomical variations of the arterial supply of the liver are reported to occur in 25-50% of the total population [3].
The most common variations of the left hepatic artery (LHA) origin are: from left gastric artery (LGA) - 25% [4, 5], splenic and gastroduodenal artery - 4% [6] and directly from the aorta - 0.5- 2% [6-9].
Our goal is to highlight the importance of knowing the hepatic artery anatomy and its variations since we have found an exceptional replaced LHA arising from the superior mesenteric artery (SMA).
MATERIAL AND METHODS
Human cadaver livers (n=60) were obtained from routine autopsies. The cadavers and the livers had to comply with the following requirements: (1) minimum age 18 years old, (2) no liver pathology to be expected from medical history and, (3) no liver pathology noted at the autopsy.
The Research and Ethical Committee of the University of Sao Paulo School of Medicine approved the human cadaver research.
Resections were carried out en bloc with liver, celiac axis, left gastric artery, lesser omentum, superior mesenteric artery and pancreas head. An eventual left or right hepatic artery was thus taken down in continuity with the aorta. The liver was dissected free from its peritoneal attachments. The hepato-duodenal ligament was dissected as close to the duodenum as possible. The gallbladder, if present, was removed.
In the division of right and left lobes of the liver it was necessary to excise the caudate lobe (segment I). The cutting plane of the liver consisted of a longitudinal section made immediately on the left of the supra-hepatic inferior vena cava through the gallbladder bed preserving the arterial, portal and biliary branches in order to obtain two viable grafts (right lobe - segments V,VI,VII,VIII and left lobe - segments II,III,IV) as defined by the main portal scissure. The hepatic artery was dissected out and recorded carefully when the liver was split in right and left lobe.
RESULTS
We have found right and left hepatic artery in 45(75%) cases; replaced or accessory LHA arising from the LGA in 9(15%) cases; replaced or accessory right hepatic artery (RHA) originating from the SMA in 4(6.6%) cases; the right hepatic artery coming from the SMA in 15 (25%) cases; the left hepatic artery originating from the LGA in 2 (3.3%) cases; the entire CHA arising as a branch of the SMA in 1 (1.6%) case; the CHA originating directly from the aorta in 11(18.3%) cases; accessory RHA from SMA and replaced LHA from LGA in 3(5%) cases; replaced RHA and LHA from SMA in 1(1.6%) case; LHA arising directly from the aorta in 1(1.6%) case.
One case had an exceptional anatomic variation, replaced LHA coming off the SMA directly to the hepatic left lobe (Fig. 1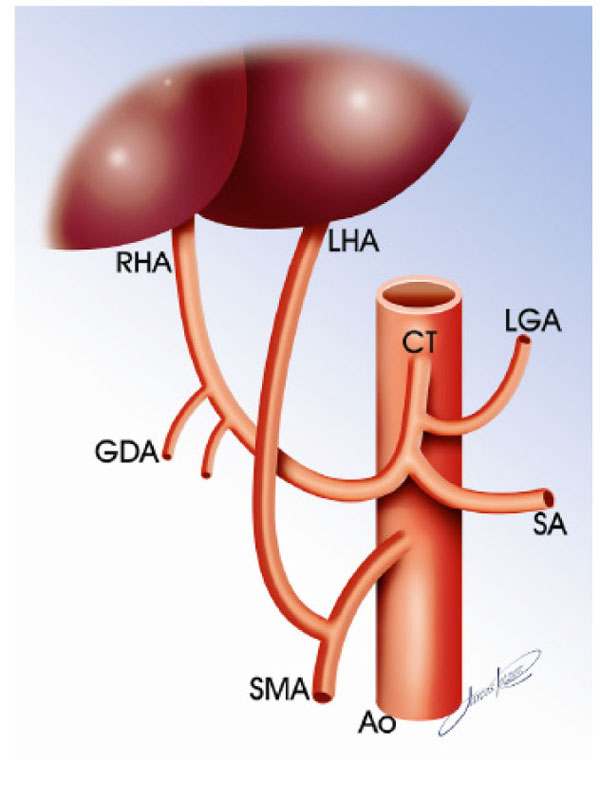 ).
).

DISCUSSION
Anatomical variations of the arterial supply of the liver are not uncommon. Only half of the cases in anatomical studies have the typical normal anatomy of the hepatic artery [10, 11]. Some of the variations such as the presence of a right or left hepatic branch arising from SMA and LGA respectively are more common, but others also relating to blood supply of the liver are extremely rare [12, 13].
Michels [5] reported a classification of 10 possible anatomical variants of the extra-hepatic arterial distribution that was based on a study of 200 autopsy cases. From a surgical point of view the classification is more complete since it establishes the differences between “an accessory” and “a replaced” artery, concepts not explained in more recent classifications.
Replaced hepatic arteries are anomalies that are easily managed, in contrast, the presence of accessory arteries might result in reconstructions of double arteries that, because of their small diameters, are the cause of an increased rate of arterial thrombosis in liver transplantation procedure despite the use of refined suture techniques [14, 15].
This study found that the LHA arose from the LGA in 10 (16.6%) cases, according to literature replaced or accessory LHA range from 9.7 to 12% [16]. In one (1.6%) case the CT arose from the SMA, this specific anatomical variation range from 1.1 to 1.5% [16].
LHA originating directly from the SMA as replaced artery is extremely rare anatomic variation, its incidence when originated from aorta range from 0.5 to 2% [12, 13]. Abdominal arteries arising from the superior mesenteric artery is shown in the Table 1. Moreover, the hepatic artery arising from the hepatic-mesenteric trunk and crossing the portal vein anterior to it has been described elsewhere [13].
Embryological CT and the SMA may have a common origin from the aorta (incidence approximately 1%) or the trunk may have become a fibrotic string [4, 9]. The arc of Buhler, i.e. a link vessel between the hepatic artery and the SMA, is not so unusual [4, 10], a seemingly more extraordinary situation is the case where a strong communicating artery between the CT and the SMA was found, on the other hand the RHA off the SMA occurs in up to 20% of all cases [2].
According to the theory of Tandler [17], the CA and the SMA develop as cephalic roots of vitelline or omphalo-mesenteric arteries, which are joined with a ventral para-aortic anastomosis between the 4th and 7th gestational weeks.
The embryological development of the liver starts in the 3rd gestational week as a hepatic diverticulum of the foregut [18]. The dorsal arteries join to form the aorta, from which paired branches provide a supply of blood to both the foregut and the liver bud. Since the primitive vitelline arteries form the CT and the SMA, one of these paired branches to the left of the foregut seems to have persisted in our case, creating a branch that irrigate the left lobe of the liver.
In conclusion, we would like to draw attention for this particularly anatomic variation of the origin of the LHA ensuring that no damage will be made during gastrointestinal surgery.