- Home
- About Journals
-
Information for Authors/ReviewersEditorial Policies
Publication Fee
Publication Cycle - Process Flowchart
Online Manuscript Submission and Tracking System
Publishing Ethics and Rectitude
Authorship
Author Benefits
Reviewer Guidelines
Guest Editor Guidelines
Peer Review Workflow
Quick Track Option
Copyediting Services
Bentham Open Membership
Bentham Open Advisory Board
Archiving Policies
Fabricating and Stating False Information
Post Publication Discussions and Corrections
Editorial Management
Advertise With Us
Funding Agencies
Rate List
Kudos
General FAQs
Special Fee Waivers and Discounts
- Contact
- Help
- About Us
- Search


The Open Clinical Cancer Journal
(Discontinued)
ISSN: 1874-1894 ― Volume 5, 2011
Expression of Nuclear β-Catenin in Rectal Versus Colonic Cancers
Rolf Aamodt*, 1, Johan Bondi1, Solveig Norheim Andersen2, Geir Bukholm3 , Ida R.K. Bukholm1
Abstract
Rectal cancers have more local relapses than colonic cancers. Since nuclear β-catenin plays an important role for the proliferation capacity of cells, we wanted to evaluate whether there may be differences in the expression pattern of nuclear β-catenin between rectal and colonic adenocarcinomas, explaining the observations made in clinical practice. Sec- tions from 235 rectal adenocarcinomas treated surgically in the years 1992 - 2000 were immunohistochemically stained for β-catenin. Nuclear immunopositivity was recorded. The results were compared to the results of a similar examination performed earlier on 162 colonic cancers. We found a higher protein expression of nuclear β-catenin in rectal cancers than in colonic cancers. No statistically significant correlation was observed between nuclear expression of β-catenin in rectal cancers and cancer specific survival. Our findings indicate that rectal cancers and colonic cancers are biologically different. The results might partly explain the clinical difference observed between rectal cancers and colonic cancers.
Article Information
Identifiers and Pagination:
Year: 2008Volume: 2
First Page: 13
Last Page: 17
Publisher Id: TOCCJ-2-13
DOI: 10.2174/1874189400802010013
Article History:
Received Date: 5/12/2007Revision Received Date: 7/12/2007
Acceptance Date: 28/1/2008
Electronic publication date: 18/3/2008
Collection year: 2008
open-access license: This is an open access article licensed under the terms of the Creative Commons Attribution Non-Commercial License(http://creativecommons.org/licenses/by-nc/3.0/), which permits unrestrictive use, distribution, and reproduction in any medium, provided the original work is properly cited.
* Address correspondence to this author at the Department of Surgery, Akershus University Hospital, 1478 Loerenskog, Norway; E-mail: rolf.aamodt@medisin.uio.no
| Open Peer Review Details | |||
|---|---|---|---|
| Manuscript submitted on 5-12-2007 |
Original Manuscript | Expression of Nuclear β-Catenin in Rectal Versus Colonic Cancers | |
INTRODUCTION
Adenocarcinomas of the rectum and colon can be different with regard to the cellular biological basis for cancer development.
This view is in conflict with the readily observable fact that adenocarcinomas of the colon and the rectum have the same appearance both macroscopically and microscopically. The location of the border between the two organs is not obvious. It is therefore usually defined either by a fixed length from the anal verge regardless of body size, or by its relation to the promontory of the sacrum. These facts support the traditional view that adenocarcinoma of the rectum and colon is in fact the same disease that has just happened to strike at different anatomical level.
However, clinical observations indicate that there can be biological differences between these two localizations. Adenocarcinomas located within the rectal cavity have a higher local recurrence rate and a lower rate of distant and peritoneal metastases than colonic cancers [1-5]. The incidence of lymph node metastasis has been shown to be higher in rectal tumors than in colonic tumors [6,7] and the risk of lymph node metastases increases from proximal to distal direction of the rectal cavity [8]. The beneficial effect of adjuvant chemotherapy is larger in colonic cancers than in rectal cancers [9]. The effect of radiotherapy also differs between colonic and rectal adenocarcinomas [10].
Local relapse, distant metastases, the effect of treatment and the prognosis of cancer patients depend on the biology of the tumor. Hence, we hypothesize that molecular biological differences are responsible for the differences in clinical behavior between colonic and rectal adenocarcinomas. There are few studies where the molecular biological differences between colonic and rectal adenocarcinomas have been investigated [4, 11, 12].
Abnormally located β-catenin plays a central role in colorectal tumorigenesis [13] by being part of the signalling cascade of the Wnt pathway [14]. β-catenin plays its key role in tumorigenesis in association with APC [15,16]. Mutations in either β-catenin or APC can distort the normal tumor suppressive effect of APC [15]. Somatic mutations of the APC gene causes malfunctioning APC in 80 % of colorectal cancers [13]. This malfunctioning APC fails to reduce the level of cytoplasmic β-catenin [13,17]. The resulting increased level of cytoplasmic β-catenin induces transcription through the TCF/LEF pathway [13], leading to increased proliferation rate of the cancer cells.
Many studies have been performed on different aspects of the relation between β-catenin and colorectal tumors, but few have investigated the expression patterns of β-catenin in rectal carcinomas and made comparison to the findings in colonic cancers [3,18].
The aim of the study was to compare the expression pattern of β-catenin between colonic and rectal adenocarcinomas.
MATERIALS AND METHODOLOGY
All available tumor samples from a consecutive series of 274 paraffin-embedded rectal adenocarcinomas removed surgically at Akershus University Hospital in the years 1992 – 2000 were scrutinized for inclusion into the survey. These surgical treatments were all primary operations. We decided to include solely tumors at a level of 15 centimeters (5.9 inches) or less from the anal verge (i.e. the outer border of the anus). This level was chosen partly because this is a commonly used definition of the border between the rectum and the colon. We wanted a restrictive border in order to avoid unintentional inclusion of sigmoid tumors.
This material of rectal carcinomas was compared to a material by Bondi et al. of 162 colon carcinomas operated on at Akershus University Hospital during the years 1988, 1990 and 1997-2000 [19].
Immunohistochemistry
Sections (3 - 4 micrometers) from formalin fixed, paraffin wax embedded archive tumor tissue were applied to coated slides. After antigen retrieval by microwaving (20 min at 100 degrees Celsius), immunostaining with anti-β-catenin (Novocastra Laboratories, Newcastle upon Tyne, UK, dilution 1:300) was performed in Autostainer (Dako Corporation, Carpentaria, USA), according to the operation protocol. The antibody was visualized for light microscopy with Envision Plus-System and diaminobenzidine (DAB). Counter-staining was done with Hagen’s haematoxylin for visualization of tissue structures. Positive control was a test block with multiple colonic adenocarcinomas with diverse differentiation.
We counted the percentage of positive nuclei semi quantitatively by applying four grades of immunopositivity, 0, 1, 2 and 3. Only nuclear staining was recorded. When 60 % or more of the nuclei were stained, we scored the tumor as grade 3 (Fig. 3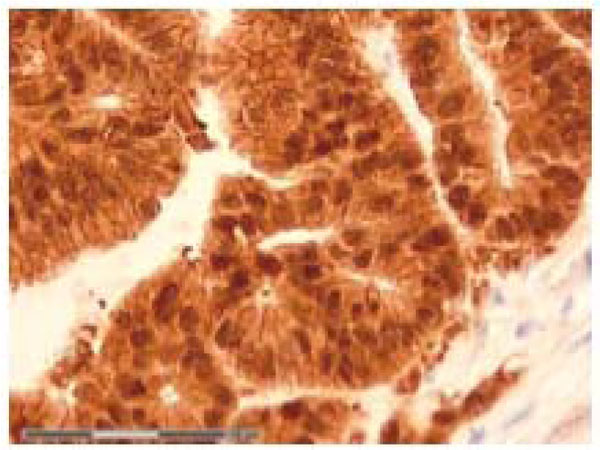 ). Staining of 30 % up to 60 % of the nuclei was classified as grade 2 (Fig. 2
). Staining of 30 % up to 60 % of the nuclei was classified as grade 2 (Fig. 2 ). When nuclear staining was less than 30 %, the score was grade 1 (Fig. 1
). When nuclear staining was less than 30 %, the score was grade 1 (Fig. 1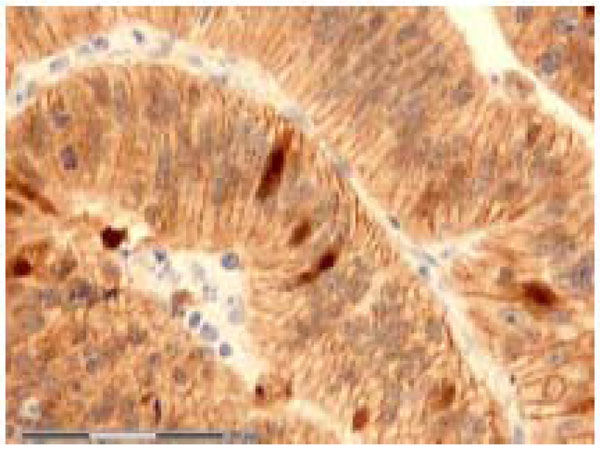 ). No nuclear immunostaining at all qualified for grade 0 (Fig. 4
). No nuclear immunostaining at all qualified for grade 0 (Fig. 4 ). Only clearly nuclear staining was recorded as positive. Almost all slides contained normal adjacent mucosa in addition to the cancer. The normal mucosa served as an internal control. The slides were judged independently by three investigators (RAa, IRKB and JB). At least 100, usually more than 1000 cells were examined in each slide.
). Only clearly nuclear staining was recorded as positive. Almost all slides contained normal adjacent mucosa in addition to the cancer. The normal mucosa served as an internal control. The slides were judged independently by three investigators (RAa, IRKB and JB). At least 100, usually more than 1000 cells were examined in each slide.
 |
Fig. (1) Grade 1 immunostaining of nuclear β-catenin in rectal adenocarcinoma. Original magnification 40 X. |
 |
Fig. (2) Grade 2 immunostaining of nuclear β-catenin in rectal adenocarcinoma. Original magnification 40 X. |
 |
Fig. (3) Grade 3 immunostaining of nuclear β-catenin in rectal adenocarcinoma. Original magnification 40 X. |
 |
Fig. (4) Grade 0 immunostaining of nuclear β-catenin in rectal adenocarcinoma. Original magnification 40 X. |
The slides of the colonic material of Bondi et al. were produced and classified in the same way [19].
Statistical Analyses
Statistical analyses were performed by SPSS version 14.0 running on Windows XP. Binary logistic regression analysis was used to evaluate the levels of β-catenin expression in rectal cancers compared to colonic cancers. This comparison was also done by means of one-way ANOVA. Survival analyses were carried out by Cox regression. Test plot for proportional hazard was performed. We chose an alpha level of statistical significance of p<0.05.
RESULTS
Table 1 shows the main characteristics of the rectal cancers.

The tumors were classified according to Dukes’ classification of 1932 with the addition of a class D introduced by Turnbull et al. in 1967 [20] in such a way that the Dukes A, B, C and D classes correlate to the stages I, II, III and IV based on the TNM-classification [21]. The TNM classification of each cancer was also recorded. Patients were followed up according to the Norwegian guidelines for colorectal patients for five years after surgery.
Mean follow-up time for the rectal cancers was 6.01 years, median 6.09, ranging from 0.01 to 14.53 years, standard deviation 4.16. One hundred and thirty-two patients (56.2 %) died during follow-up. Out of these, 53 (40.2 %) died from rectal cancer. Twenty-three cancers (9.8 %) recurred locally. In 47 patients (20.0 %), distant metastasis was discovered during follow-up, at a later time than surgery. Mean time from surgery till local relapse was 2.26 years. Mean time from surgery till distant metastasis was 2.32 years. Mean time from surgery till local relapse and/or distant metastasis was 2.11 years.
In the colon material, 4 cancers (2.5 %) were T1, 24 (14.7 %) T2, 126 (77.3 %) T3 and 8 (4.9 %) T4. I.e. there was a tendency towards lower T stages in the rectal cancers. The percentage of Dukes’ A cancers was three times higher in the rectal material than in the colon material. A slight majority of the colon cancer patients were females while the opposite was true for the rectal cancers. The rectal patients were slightly younger than the colon patients.
From a total of 274 rectal carcinomas, 235 were available for evaluation of β-catenin protein expression.
The results of the immunostaining of nuclear β-catenin are shown in Table 2.

When comparing the expression level of nuclear β-catenin between colonic and rectal adenocarcinomas by means of one-way ANOVA analysis, we observed a highly significant difference between rectal adenocarcinomas and colonic adenocarcinomas (p < 0.00001). The post hoc tests of the ANOVA analysis indicated that the difference between colon and rectum was larger when β-catenin had an immunopositivity of grade 0 or 1 than when the grade was 2 and 3.
The same comparison was also performed by means of binary logistic regression analysis. In this analysis we adjusted for Dukes stage, patient age, T-stage, and tumor differentiation grade. This analysis also showed a highly significant difference between rectal and colonic cancers concerning the expression level of nuclear β-catenin (p< 0.00001. OR=31.7, 95 % CI for OR [16.8; 59.9]). The nuclear expression of β-catenin was higher in rectal compared to colonic adenocarcinomas. None of the other parameters included in the analyses, except T-stage, showed any statistical difference between colonic and rectal adenocarcinomas. The T-stage was higher in the colonic adenocarcinomas than in the rectal adenocarcinomas (p=0.009, OR=0.452, 95 % CI for OR [0.250; 0.818]).
No statistically significant correlation was observed between nuclear expression of β-catenin in rectal cancer and cancer specific survival, distant metastasis nor local relapse of the cancer.
DISCUSSION
We found a higher protein expression of nuclear β-catenin in rectal cancers than in colonic cancers. The difference was highly significant.
The percentage of nuclear β-catenin expression was higher in the present study than in previously published data. We observed nuclear β-catenin expression in 94.9 % of the tumors, which is higher than observed in studies performed by Gunther et al. [18] and Kapiteijn et al. [3]. The reason for this discrepancy is difficult to explain exactly, but it is possible that the composition of patient groups between these studies may have been different regarding tumor stage.
The lack of association between rectal nuclear β-catenin expression and clinical outcome observed in the present study is in concordance with the observations of Gunther et al. [18]. In contrary, Cheach et al. [22] found a significant relation between nuclear β-catenin expression and higher mortality rates. Their patients were colorectal cancer patients, i.e. a mixture of colonic and rectal cancers. Bondi et al. [19] found a borderline association between the same parameters in their examination of exclusively colonic cancers. We believe that a relationship between nuclear β-catenin expression and mortality seems to exist for some colonic cancers. This relation appears to be lacking in rectal cancers.
Increased translocation of β-catenin to the nucleus of tumor cells is usually the result of reduced degradation of cytosolic β-catenin. The APC gene plays an important role in the degradation of β-catenin [13,17], and mutation in either the APC gene or in the β-catenin gene itself may lead to reduced degradation and increased translocation to the nucleus. Dimberg et al. detected higher prevalence of mutations in the mutation cluster region of the APC gene in rectal cancers than in colonic cancers. Their investigation also indicated a relation between APC mutations in human colorectal cancers and nuclear translocation of β-catenin [23]. From this, one might suspect a higher prevalence of nuclear β-catenin in rectal cancers than in colonic cancers, as observed in the present study.
Translocated β-catenin leads to increased expression of cyclin D1 [24] and c-Myc [25], which may turn up the proliferation capacity of the tumor cells. Tumor cells with high proliferation rate may expand locally fast, escaping from the immune system. This can cause a local recurrence that is of clinical significance. The results from the present study support, and in part explain why local relapse may be a more pronounced problem in rectal cancer. The results may also partly explain the necessity of not leaving any cancer behind when doing surgery. A few rectal cancer cells left behind can multiply rapidly because of the high proliferation rate of the tumor cells, leading to clinically significant local recurrence.
Local relapse was a major problem before the introduction of TME (total mesorectal excision) as a standard procedure. After the introduction of TME the local relapse frequency of rectal cancer is declining [26], probably because of better salvage of tumor cells by the TME procedure.
A more rapid growth of a localized tumor does not necessarily lead to more distant metastases. This may be why there is no significant association between nuclear expression of β-catenin and cancer specific survival. Rectal cancer patients die from distant metastasis and not from a localized tumor in the pelvic cavity alone. If handled correctly, a local relapse need not necessarily lead to mortality, but is associated with high morbidity.
CONCLUSION
We have in the present study observed a highly significant difference in nuclear expressed β-catenin between colonic and rectal adenocarcinomas, even when adjusted for other histopathological and clinical parameters. This difference in the cellular biology between these two localizations may in part explain the differences observed in clinical practice.
ACKNOWLEDGEMENTS
The study and the manuscript preparation were funded by the South-Eastern Norway Regional Health Authority and the University of Oslo.