- Home
- About Journals
-
Information for Authors/ReviewersEditorial Policies
Publication Fee
Publication Cycle - Process Flowchart
Online Manuscript Submission and Tracking System
Publishing Ethics and Rectitude
Authorship
Author Benefits
Reviewer Guidelines
Guest Editor Guidelines
Peer Review Workflow
Quick Track Option
Copyediting Services
Bentham Open Membership
Bentham Open Advisory Board
Archiving Policies
Fabricating and Stating False Information
Post Publication Discussions and Corrections
Editorial Management
Advertise With Us
Funding Agencies
Rate List
Kudos
General FAQs
Special Fee Waivers and Discounts
- Contact
- Help
- About Us
- Search


The Open Leukemia Journal
(Discontinued)
ISSN: 1876-8164 ― Volume 5, 2013
Feasibility and Outcome of Allogeneic Hematopoietic Stem Cell Transplantation in 30 Patients with Poor Risk Acute Myeloid Leukemia Older than 60 Years
Candoni Anna*, Simeone Erica, Cerno Michela, Sperotto Alessandra , Fanin Renato
Abstract
We report on the feasibility and outcome of allogeneic SCT (allo-SCT) in 30 poor risk AML patients older than 60 years. Median age at transplant was 63 years (range 60-70 years) and 18/30 (60%) cases were in complete remission. Donors were MUD in 40% and sibling in 60% of cases. Twenty-six of 30 patients (87%) received a reduced intensity conditioning regimen (RIC). The hematopoietic cell transplantation specific comorbidity index (HCT-CI) was two or less in 12/30 cases and three or more in 18/30 cases. All patients engrafted. One year Nonrelapse mortality (NRM) rate was 20% (6/30 cases). After a median follow-up of 16 months 17/30 patients (57%) were alive and in complete remission while 13/30 (43%) have died (leukemia refractory or relapse 7/13 and NRM 6/13). Median Overall Survival for the whole patient population was 28 months. The Overall Survival did not differ between unrelated and related donors. The patients transplanted in complete remission had a significantly lower survival rate and relapse rate compared to those transplanted with refractory or relapsed AML (P= 0.0004 and P= 0.008 respectively). The patients with a low HCT-CI (2 or less) had a significantly lower NRM (P = 0.03) and survival rate (P = 0.02) compared to those with HCT-CI 3 or more.
Taking into account that this is a retrospective analysis with a small number of cases, these results confirm the feasibility of allo-SCT for high risk AML patients older than 60 years. Outcome was significantly influenced by status of disease at transplant and by HCT-CI. We also confirm that for older patients lacking a family donor MUD can provide a suitable alternative option.
Article Information
Identifiers and Pagination:
Year: 2010Volume: 3
First Page: 55
Last Page: 59
Publisher Id: TOLEUKEMIAJ-3-55
DOI: 10.2174/1876816401003010055
Article History:
Received Date: 31/5/2010Revision Received Date: 21/7/2010
Acceptance Date: 26/7/2010
Electronic publication date: 8/9/2010
Collection year: 2010
open-access license: This is an open access article licensed under the terms of the Creative Commons Attribution Non-Commercial License (http: //creativecommons.org/licenses/by-nc/3.0/ which permits unrestricted, non-commercial use, distribution and reproduction in any medium, provided the work is properly cited.
* Address correspondence to this author at the Division of Hematology and Bone Marrow Transplantation Unit, University of Udine, Italy; Tel: 0432-559662; Fax: 0432 559661; E-mail: candoni.anna@aoud.sanita.fvg.it
| Open Peer Review Details | |||
|---|---|---|---|
| Manuscript submitted on 31-5-2010 |
Original Manuscript | Feasibility and Outcome of Allogeneic Hematopoietic Stem Cell Transplantation in 30 Patients with Poor Risk Acute Myeloid Leukemia Older than 60 Years | |
INTRODUCTION
Older age is one of the most important adverse prognostic factors in Acute Myeloid Leukemia (AML) [1Appelbaum FR, Gundacker H, Head DR, et al. Age and acute myeloid leukemia Blood 2006; 107: 3481-5.,2Deschler B, De Witte T, Mertelsmann R, et al. Treatment decision making for older patients with high-risk myelodysplastic syndrome or acute myeloid leukemia: problems and approaches Haematologica 2006; 91: 1513-22.]. Allogeneic stem cell transplantation (allo-SCT) is one of the most recommended approaches in poor prognosis AML but there are limited data about this procedure in elderly AML patients [1Appelbaum FR, Gundacker H, Head DR, et al. Age and acute myeloid leukemia Blood 2006; 107: 3481-5.-4Kiss TL, Sabry W, Lazarus HM, et al. Blood and marrow transplantation in elderly acute myeloid leukaemia patients: older certainly is not better Bone Marrow Transplant 2007; 40: 405-16.]. The results of allo-SCT seem to be improved in terms of lower transplant related toxicity with the development of so-called reduced intensity conditioning (RIC) regimens. The introduction of RIC transplant has increased the percentage of AML candidate to allo-SCT procedure [5Bertz H, Potthoff K, Finke J. Allogeneic stem-cell transplantation from related and unrelated donors in older patients with myeloid leukemia J Clin Oncol 2003; 21: 1480-4.,6Shimoni A, Kroger N, Zabelina T, et al. Hematopoietic stem-cell transplantation from unrelated donors in elderly patients (age > 55 years) with hematologic malignancies older age is no longer a contraindication when using reduced intensity conditioning Leukemia 2005; 19: 7-12.]. Nevertheless, most of the largest studies reported in the literature with RIC or conventional regimes in older than 60 years include cases with heterogeneous clonal hematopoietic disorders (a mix of acute and chronic myeloid leukemia and lymphomas).
We report on our experience about the feasibility and the outcome of the allo-SCT from a series of 30 AML patients older than 60 years.
PATIENTS AND METHODS
Between 1 January 2004 and 31 December 2009, 30 patients aged over 60 years with AML underwent allo-SCT at our Centre. Baseline patient characteristics are reported in Table 1. All 30 cases were at high risk at diagnosis because of therapy related or secondary AML, unfavourable karyotype (-5, -7, 11q23, complex karyotype) or a blast count > 30 x 109/l. Donor-search, either within the family or in volunteer donor Registries worldwide, was performed during induction chemotherapy. All patients provided written informed consent for transplantation protocols that were approved by the institution Ethic Committee. The hematopoietic cell transplantation specific comorbidity index (HCT-CI) was two or less in 12/30 cases (40%) and three or more in 18/30 cases (60%).
Allo-SCT conditioning regimens were employed according the national ongoing trials. Conditioning regimen consisted of Thyotepa + Cyclophosphamide ± ATG in 14/30 (47%) of cases, Fludarabine-based RIC in 12/30 (40%) of cases, Busulfan + Cyclophos-phamide ± ATG in 4/30 (13%) of cases. Twenty-six of 30 patients (87%) received a reduced intensity conditioning regimen (RIC) and 4 (13%) a myeloablative one (Table 1). Graft Versus Host Disease (GvHD) prophylaxis consisted of intravenous cyclosporine (3-5 mg/kg) and methotrexate (10 mg/m2 on days 1, 3, 6 and 11). One patient received cyclosporine alone and one received cyclosporine in combination with mycophenolate mofetil (MMF). Cyclosporine was given orally as soon as the patients were able to swallow. Matched unrelated donor (MUD) recipients received also anti-T lymphocyte globulin 40 to 60 mg/kg body weight (ATG-S; Fresenius, Grafelfing, Germany). Patients were housed in rooms with HEPA-filtered air. All patients received prophylactic anti-microbial therapy with levofloxacine and fluconazole from admission until engraftment. Toxicities were graded according to the World Health Organization (WHO) criteria [7Miller AB, Hoogstraten B, Staquet M, et al. Reporting results of cancer treatment Cancer 1981; 47: 207-14.]. Acute and chronic GvHD were graded and staged by standard criteria [8Przepiorka D, Weisdorf D, Martin P, et al. 1994 Consensus Conference on Acute GVHD Grading Bone Marrow Transplant 1995; 15: 825-.]. Neutrophil and platelet recovery were defined as the first of two consecutive days with Absolute Neutrophil Count (ANC) > 1 x 109/l and platelets (PTL) > 50 x 109/l without transfusions, respectively. Chimerism was tested after 1 month and at 3 month intervals with PCR analysis of microsatellite markers [9Thiede C, Bornhauser M, Oelschlagel U, et al. Sequential monitoring of chimerism and detection of minimal residual disease after allogeneic blood stem cell transplantation (BSCT) using multiplex PCR amplification of short tandem repeat-markers Leukemia 2001; 15: 293-302.]. AML response and relapse were determined by standard hematologic criteria [10Cheson BD, Bennett JM, Kopecky KJ, et al. Revised recommendations of the international Working Group for Diagnosis, Standardization of response Criteria. Treatment Outcomes. and reporting Standards for therapeutic Trials in acute myeloid leukemia J Clin Oncol 2003; 21: 4642-9.].
Overall survival (OS) was computed from transplant date until death or last follow-up. Patient’s last follow-up was march 31, 2010. Survival curves were constructed using the Kaplan-Meier method. Patient’s characteristics were compared by the Fisher’s exact test for categoric variables. P-value less than 0.05 was considered as statistical significant. Data were analysed using NCSS60 software (NCSS Company, Kaysville, UT, USA).
RESULTS
1. Transplantation Details and Engraftment
The median time from diagnosis to transplant was 7 months. The median age at transplant was 63 years (range 60-70) and 13 patients (43%) were older than 65 years. At the time of transplantation, 18 cases (60%) were in complete remission (CR), while 12 (40%) had an active disease (relapsed or refractory AML). The comorbidities included: hypertension (9 patients), diabetes mellitus (3 patients), stable heart diseases (5 patients), hepatic or renal diseases (3 patients). Besides 8 patients had a prior history of solid tumours that required chemotherapy (of which 2 had multiple tumours). Eighteen patients (60%) received an allograft from a sibling, 12 (40%) from an unrelated donor. The median age of sibling donors was 63 years (range 39-73) compared to 39 years (range 27-48) of unrelated donors (P < 0.05). Stem cell source was bone marrow (BM) in 11 (37%) and unmanipulated peripheral blood (PB) in 19 (63%) patients. Median number of CD34+ cells was 5 x 106/kg body weight (range 0,8-18.5), significantly higher in PB than in BM recipients (6.5 vs 1.6 x 106/kg, P < 0.05).
All patients became neutropenic (ANC < 0.5x109/l) and thrombocytopenic (PLT < 20x109/l), requiring a median of 4 platelet transfusions (range, 1-30) and a median of 7 erythrocyte transfusions (range, 1-30). All patients engrafted. The median time to neutrophil and platelet recovery was 18 (range 12-31) and 19 days (range 10-60), respectively, without differences according to stem cell source (BM or PB) (Table 2). Chimerism analysis was available in 25/30 cases: at the first testing after engraftment (day 35), 17/25 (68%) patients had complete donor chimerism and 8/25 (32%) had mixed chimerism (60% to 98% donor). Data were not available for 5 patients: two died early, two had persistent leukemia and 1 was not tested for other reasons.
2. GvHD, Toxicity and Outcome
As presented in Table 2, all 30 patients were assessable for acute GvHD. Acute GvHD was observed in 17/30 patients (56%) with 13 having grades I-II and 4 having grades III-IV. Data on chronic GvHD was available for 22/30 patients (73%); of those 2/22 (9%) experienced extensive chronic GvHD requiring prolonged immunosuppressive therapy and 9/22 (41%) had limited chronic GvHD. Data summarizing haematological recovery, transfusion support and more relevant toxicity are reported in Table 2. Grade 3-4 mucositis occurred in 5/30 (17%) patients. Infections occurred in 16 patients (53%), including 14 cases of bacteraemia and 9 cases of pneumonia (4 bacteria, 3 aspergillus, 1 Pneumocystis and 1 Cytomegalovirus). Infectious death occurred in 3 patients who developed pneumonia, septic shock and multi-organ failure. No cases of Veno Occlusive Disease were reported. One year Nonrelapse mortality (NRM) rate was 20% (6/30 cases). Causes of NRM were: pneumonia with septic shock (n=1), acute GvHD (n=3), sudden cardiac death (1), and intracranial haemorrhage (n=1). The median length of hospital stay, for allo-SCT, was 40 days (range 28-90).
At the time of analysis, after a median follow-up of 17 months (range 1-64), 17/30 patients (57%) were alive and in complete remission while 13/30 (43%) have died (leukemia refractory or relapse 7/13 and NRM 6/13). The median follow-up for transplant survivors was 27 months (range 2-64). Median Overall Survival (OS) for the whole patient population was 28 months (Fig. 1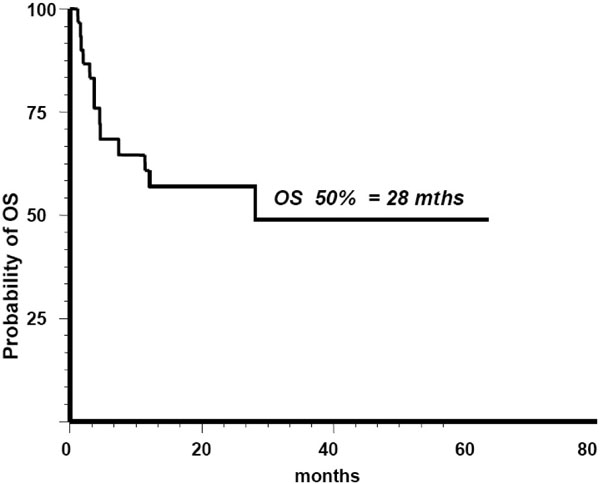 ). One year probability of Overall Survival (OS) was 57% (95% CI: 24% to 81%). The OS and toxicity did not differ between sibling and MUD recipients. The patients transplanted in complete remission have a significantly better survival rate (P = 0.0004) and lower relapse rate (P= 0,008) compared to those transplanted with active AML (Table 3). The patients with a low HCT-CI (2 or less) have a significantly better survival rate (P = 0.02) and lower Non Relapse Mortality (NRM) (P=0.03) compared to those with HCT-CI 3 or more (Table 3).
). One year probability of Overall Survival (OS) was 57% (95% CI: 24% to 81%). The OS and toxicity did not differ between sibling and MUD recipients. The patients transplanted in complete remission have a significantly better survival rate (P = 0.0004) and lower relapse rate (P= 0,008) compared to those transplanted with active AML (Table 3). The patients with a low HCT-CI (2 or less) have a significantly better survival rate (P = 0.02) and lower Non Relapse Mortality (NRM) (P=0.03) compared to those with HCT-CI 3 or more (Table 3).
 |
Fig. (1) Median Overall Survival (OS) of The whole Population after Allo-SCT was 28 months. |
DISCUSSION
The incidence of acute myeloid leukemia (AML) increases with age and over half of the AML patients at diagnosis are older than 60 years [1Appelbaum FR, Gundacker H, Head DR, et al. Age and acute myeloid leukemia Blood 2006; 107: 3481-5.,2Deschler B, De Witte T, Mertelsmann R, et al. Treatment decision making for older patients with high-risk myelodysplastic syndrome or acute myeloid leukemia: problems and approaches Haematologica 2006; 91: 1513-22.]. Despite improvements in chemotherapy and supportive care, the prognosis of AML patients older than 60 years remains poor and cure is rarely achieved using conventional chemotherapy (with 2 year disease free survival rates lower than 20%) [1Appelbaum FR, Gundacker H, Head DR, et al. Age and acute myeloid leukemia Blood 2006; 107: 3481-5.,2Deschler B, De Witte T, Mertelsmann R, et al. Treatment decision making for older patients with high-risk myelodysplastic syndrome or acute myeloid leukemia: problems and approaches Haematologica 2006; 91: 1513-22., 11Shapira MY, Tsirigotis P, Resnick IB, et al. Allogeneic hematopoietic stem cell transplantation in the elderly Crit Rev Oncol Hematol 2007; 64: 49-63.]. Allogeneic hematopoietic stem cell transplantation (allo-SCT) is a curative option, but the issues of its safety and efficacy in elderly patients are still under debate [11Shapira MY, Tsirigotis P, Resnick IB, et al. Allogeneic hematopoietic stem cell transplantation in the elderly Crit Rev Oncol Hematol 2007; 64: 49-63., 12Blaise D, Vey N, Faucher C, et al. Current status of reduced intensity conditioning allogeneic stem cell transplantation for acute myeloid leukemia Haematologica 2007; 92: 533-41.]. In fact the risk of Nonrelapse mortality (NRM) increases with age, particularly after 55-60 years. The development of reduced intensity conditioning (RIC) regimens has upraised the age limit for allo-SCT over 60 years, mainly by reducing the impact of NRM [11Shapira MY, Tsirigotis P, Resnick IB, et al. Allogeneic hematopoietic stem cell transplantation in the elderly Crit Rev Oncol Hematol 2007; 64: 49-63.-13Appelbaum FR. What is the impact of hematopoietic cell transplantation (HCT) for older adults with acute myeloid leukaemia (AML)? Best Pract Res Clin Haematol 2008; 21: 665-7.]. The studies reported in the literature with RIC or conventional regimes in patients aged ≥ 60 years are rare and include cases with heterogeneous clonal hematopoietic disorders (acute and chronic myeloid leukemia, lymphomas). As reported in Table 4 a limited data have been available regarding allo-SCT in AML patients older than 60 years [5Bertz H, Potthoff K, Finke J. Allogeneic stem-cell transplantation from related and unrelated donors in older patients with myeloid leukemia J Clin Oncol 2003; 21: 1480-4.,15Shapira MY, Resnick IB, Bitan M, et al. Low transplant-related mortality with allogeneic stem cell transplantation in elderly patients Bone Marrow Transplant 2004; 34: 155-9.-18Falda M, Busca A, Baldi I, et al. Nonmyeloablative allogeneic stem vcell transplantation in elderly patients with hematological malignanciesResults from the GITMO (Gruppo Italiano Trapianto di Midollo) multicenter prospective clinical trial Am J Hemat 2007; 82: 863-6.].
In the study by Bertz et al. 19 AML patients above the age of 60 underwent RIC-SCT from matched related and unrelated donors. The median age of patients was 64 years (range 60-70) and the majority of them had active disease. Conditioning consisted of fludarabine, melphalan, and carmustine. All patients engrafted and 13 out 19 (68%) achieved complete remission. With a median follow-up period of 825 days (range 595-1028), the OS was 68% without differences between MUD and sibling SCT. The 1-year NRM rate was 22% [5Bertz H, Potthoff K, Finke J. Allogeneic stem-cell transplantation from related and unrelated donors in older patients with myeloid leukemia J Clin Oncol 2003; 21: 1480-4.]. Shapira et al. reported 17 cases of AML, median age 62,5 years (range 60-67), conditioned with fludarabine plus busulfan, resulting in a NRM and OS of 33% and 29%, respectively, with a median follow-up of 11 months (range 8-53) [15Shapira MY, Resnick IB, Bitan M, et al. Low transplant-related mortality with allogeneic stem cell transplantation in elderly patients Bone Marrow Transplant 2004; 34: 155-9.]. Gupta et al. reported the outcome of 24 patients aged ≥ 60 with poor-prognosis myelodysplastic syndromes or AML, undergoing RIC-SCT; NRM at 100 days and after 2 years was 8% and 25%, respectively. The probability of 1 and 2 year OS was 60% an 52%, respectively [16Gupta V, Daly A, Lipton HJ, et al. Nonmyeloablative Stem Cell Transplantation for Myelodysplastic Syndrome or Acute Myeloid Leukemia in patients 60 years or older Biol Blood Marrow Transplant 2005; 11: 764-2.]. Also, the experiences by De Lima and Falda et al. suggest that allo-SCT is feasible in selected older poor prognosis AML patients [17De Lima M, Shahjahan M, Alamo J, et al. Allogeneic hematopoietic stem cell transplantation (HSCT) for patients aged 65 years or older with AML and MDS Blood 2004; 104: A 2301.,18Falda M, Busca A, Baldi I, et al. Nonmyeloablative allogeneic stem vcell transplantation in elderly patients with hematological malignanciesResults from the GITMO (Gruppo Italiano Trapianto di Midollo) multicenter prospective clinical trial Am J Hemat 2007; 82: 863-6.].
Our present experience confirms that allo-SCT may be a suitable option for elderly AML patients. In addition, it should be underlined that in our series 43% of patients were aged over 65 years. Despite that, NRM rate was low (20%) and the survival and toxicity were similar in recipient of sibling and unrelated donor SCT. Our results of a similar outcome of MUD transplantation compared with sibling transplantation may be due to the improvement (in recent years) of GvHD prevention and treatment, infection treatment and prophylaxis and could also be related to the Centre expertise [19Scheteling J, Bornhauser M, Schmid C, et al. Matched unrelated or matched sibling donors result in comparable survival after allogeneic stem-cell transplantation in elderly patients with acute myeloid leukemia: a report from the German Transplant Study Group J Clin Oncol 2008; 26: 5183-91.]. Therefore, in patients lacking a healthy sibling donor, which is likely to be a problem in this advanced-age group, a search for an unrelated donor should be rapidly started especially in cases without severe comorbidities.
Our data, in line with those from other groups, suggest that older age by itself should not be the limiting factor for proceeding to allo-SCT [5Bertz H, Potthoff K, Finke J. Allogeneic stem-cell transplantation from related and unrelated donors in older patients with myeloid leukemia J Clin Oncol 2003; 21: 1480-4., 15Shapira MY, Resnick IB, Bitan M, et al. Low transplant-related mortality with allogeneic stem cell transplantation in elderly patients Bone Marrow Transplant 2004; 34: 155-9.-18Falda M, Busca A, Baldi I, et al. Nonmyeloablative allogeneic stem vcell transplantation in elderly patients with hematological malignanciesResults from the GITMO (Gruppo Italiano Trapianto di Midollo) multicenter prospective clinical trial Am J Hemat 2007; 82: 863-6.]. In the elderly AML population the hematopoietic cell transplantation comorbidity index (HCT-CI), developed by Sorror and coworkers, should be used to estimate treatment related risk and to guide decision on allo-SCT [20Sorror ML, Sandmaier BM, Storer BE, et al. Comorbidity and Disease status Based Risk Stratification of Outcomes among patients with acute myeloid leukaemia or myelodysplasia receiving allogeneic hematopoietic cell transplantation J Clin Oncol 2007; 25: 4246-54.].
In conclusion, considering that this is a retrospective analysis with a small number of cases, these results confirm the feasibility of allo-SCT for high risk AML patients older than 60 years. In this experience NRM rate is only 20% and OS rate (1 year 57%) is promising taking into account the poorer outcome of elderly AML patients. Favourable outcome was observed especially in patients with a low HCT-CI (2 or less) and in those transplanted while in complete remission. We also confirm that for elderly AML patients lacking a suitable family donor MUD can provide a suitable alternative option. The evaluation of HCT-CI in elderly, before transplant procedure, could help decision making and should be considered an important part of pre transplant assessment.