- Home
- About Journals
-
Information for Authors/ReviewersEditorial Policies
Publication Fee
Publication Cycle - Process Flowchart
Online Manuscript Submission and Tracking System
Publishing Ethics and Rectitude
Authorship
Author Benefits
Reviewer Guidelines
Guest Editor Guidelines
Peer Review Workflow
Quick Track Option
Copyediting Services
Bentham Open Membership
Bentham Open Advisory Board
Archiving Policies
Fabricating and Stating False Information
Post Publication Discussions and Corrections
Editorial Management
Advertise With Us
Funding Agencies
Rate List
Kudos
General FAQs
Special Fee Waivers and Discounts
- Contact
- Help
- About Us
- Search




The Open Virology Journal
(Discontinued)
ISSN: 1874-3579 ― Volume 15, 2021
The Prognosis of Late Presenters in the Era of Highly Active Antiretroviral Therapy in Serbia
Djordje Jevtović1, Dubravka Salemović1, Jovan Ranin1, Branko Brmbolić1, Ivana Pešić-Pavlović1, Sonja Žerjav1, Olgica Djurković-Djaković*, 2
Abstract
To examine the prognosis of patients who present with very advanced HIV-induced immunodeficiency, and their response to highly active antiretroviral therapy (HAART), a series of 101 treatment naïve patients from the Serbian cohort of HIV infected patients, who presented with a CD4 count of ≤ 50/µL before commencing HAART, was retrospectively analyzed and factors influencing response to HAART and survival investigated. After a mean of three years (range 1-9) of treatment with PI-based and/or NNRTI-based regimens, a favorable response was achieved in 54.5% of the patients, treatment failure occurred in 13.9%, while 31.7% had a dissociative immunological/virological response. The overall estimated survival was eight years. Achievement of undetectable viremia during treatment appeared life saving (OR = 42.5, 95% CI 7.1 – 251.9, P = 0.000, as was a rise in CD4 cell count to over 200/μL (OR = 6.4, 95% CI 1.2- 31.8, P = 0.023). However, undetectable viremia was the single predictor of longer survival (OR = 42.5, 95% CI 7.1 – 251.9, P = 0.000), regardless of the level of immune reconstitution (log rank, P = 0.31). Late presenters had a high probability of developing the metabolic syndrome while on HAART, with a median time to hyperlipidemia and lypodystrophy of 5 and 6 years, respectively. We conclude that late presenters on HAART may have a good prognosis, a prerequisite for which is sustained undetectable viremia regardless of the immune recovery.
Article Information
Identifiers and Pagination:
Year: 2009Volume: 3
First Page: 84
Last Page: 88
Publisher Id: TOVJ-3-84
DOI: 10.2174/1874357900903010084
Article History:
Received Date: 15/6/2009Revision Received Date: 4/9/2009
Acceptance Date: 5/9/2009
Electronic publication date: 23/10/2009
Collection year: 2009
open-access license: This is an open access article licensed under the terms of the Creative Commons Attribution Non-Commercial License (http: //creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted, non-commercial use, distribution and reproduction in any medium, provided the work is properly cited.
* Address correspondence to this author at the Institute for Medical Research, University of Belgrade, Dr. Subotića 4, P.O. Box 102, 11129 Belgrade, Serbia; Tel: +381 11 2685 788; Fax: +381 11 2643 691; E-mail: olgicadj@imi.bg.ac.rs
| Open Peer Review Details | |||
|---|---|---|---|
| Manuscript submitted on 15-6-2009 |
Original Manuscript | The Prognosis of Late Presenters in the Era of Highly Active Antiretroviral Therapy in Serbia | |
INTRODUCTION
A major advance in HIV disease treatment occurred with the introduction of highly active antiretroviral treatment (HAART) in 1996. HAART regimens comprise two nucleoside reverse transcriptase inhibitors (NRTIs) and a HIV protease inhibitor (PI) or non-nucleoside reverse transcriptase inhibitor (NNRTI), potent enough for complete and prolonged cessation of viral replication to allow reconstitution of the immune system [1Jacobson MA, French MA. Altered natural history of AIDS-related opportunistic infections in the era of potent combination anti-retroviral therapy AIDS 1998; 12(A): S157-63.-3Carcelain G, Li T, Autran B. Immune reconstitution under highly active antiretroviral therapy (HAART) AIDS Rev 1999; 1: 51-6.]. Although both NRTIs and NNRTIs inhibit reverse transcriptase, their action through different mechanisms (NRTIs are phosphorylated to active metabolites and compete for incorporation into viral DNA, terminating synthesis of DNA chains, while NNRTIs bind directly to the reverse transcriptase enzyme active site) provides an enhanced effect. Immune recovery has even been achievable in severely ill patients. An overall reduction in late stage complications of HIV infection was associated with an impressive improvement in patient survival and quality of life [4Jevtovic Dj, Salemovic D, Ranin J, Pešic I, Žerjav S, Djurkovic-Djakovic O. Long-term survival of HIV-infected patients treated with highly active antiretroviral therapy in Serbia and Montenegro HIV Med 2007; 8: 75-9.-6The Antiretroviral Therapy (ART) Cohort Collaboration. Prognosis of HIV-1 infected patients up to 5 years after initiation of HAART: collaborative analysis of prospective studies AIDS 2007; 21: 1185-97.]. However, we still do witness late presenters i.e. patients diagnosed with HIV infection in the advanced stage of HIV-related immunodeficiency, when they often suffer life-threatening opportunistic infections and/or tumors [7Sabin CA, Smith CJ, Gumley H, et al. Late presenters in the era of highly active antiretroviral therapy: uptake of and response to antiretroviral therapy AIDS 2004; 18: 2145-51.-12Wong KH, Lee SS, Low KH, Wan WY. Temporal trends and factors associated with late diagnosis in Hong Kong, a low HIV prevalent locality AIDS Patient Care STDS 2003; 17: 461-9.]. Most pertinent research investigated reasons for late presentation, while some also addressed the prognosis of late presenters on HAART [5The Antiretroviral Therapy Cohort Collaboration. Life expectance of individuals on combination antiretro-viral therapy in high-income countries: a collaborative analysis of 14 cohort studies Lancet 2008; 372: 393-9.-16Rizzardi GP, Tambussi G, Bart PA, Chapuis AG, Lazzarin A, Pantaleo G. Virological and immunological response to HAART in asymptomatic therapy-naive HIV-1 infected subjects according to CD4 cell count AIDS 2000; 14: 2257-63.].
Serbia is a country of low AIDS prevalence, with, however, a low HIV-testing rate. This is why a number of patients present late in the course of HIV disease. Indeed, between January 1998 and December 2007, late presenters have accounted for 17.1% of patients referred to the national HIV/AIDS Centre. We conducted a retrospective analysis of late presenters in whom HAART was initiated to study the factors influencing response to treatment and survival.
METHODS
Patients
The study series involved 101 treatment naïve patients from the Serbian cohort of HIV infected patients treated at the HIV/AIDS Centre at the Institute for Infectious and Tropical Diseases in Belgrade, who presented between January 1998 and December 2007 with most advanced HIV-induced immunodeficiency. Inclusion criteria consisted of adult HIV infection (stages A-C according to the 1993 Centers for Disease Control case definition criteria) [17CDC. 1993 revised classification system for HIV infection and expanded surveillance case definition for AIDS among adolescents and adults MMWR 1992; 41[OR-17]: 1-19.], CD4 cell count below 50/µL (“late presenters”), and initiation on HAART after diagnosis. Follow-up was continued until the last visit, death or 31 December 2007. Patients who did not survive the index AIDS defining condition were excluded from the study. Consent for participation was obtained from all, and the study was approved by the Clinical Centre of Serbia Ethics Committee.
Demographic characteristics, AIDS diagnosis prior to HAART initiation, co-infection with hepatitis C virus (HCV), along with parameters associated with response to HAART including plasma viral load and CD4+ cell count as well as the duration of treatment, were all assessed as variables with possible influence on treatment efficacy and survival. Influence of antiretroviral drug classes used as HAART components was also analyzed.
Clinical and Laboratory Data
The immunological and virological responses to HAART were evaluated by measuring plasma viral load (pVL) and CD4+ T cell counts. Criteria for the type of response to HAART were as follows: the response was considered favorable in case of achievement of a sustained pVL reduction to undetectable values, along with CD4 cell count increases to above 200/µL. In contrast, treatment failure was defined as a pVL over 2.9 log10 copies of HIV RNA/ml of plasma regardless of immunological improvement. In addition to these two clear-cut types of response to HAART, dissociation between immunological and virological responses to HAART occurred at times, defined as achievement of undetectable viremia during treatment but without a rise in CD4 cell counts to above 200/µL [18Pakker NG, Kroon ED, Roos MT, et al. INCAS Study Group. Immune restoration does not invariably occur following long-term HIV-1 suppression during antiretroviral therapy AIDS 1999; 13: 203-12., 19Jevtovic Dj, Salemovic D, Ranin J, Pešic I, Žerjav S, Djurkovic-Djakovic O. The dissociation between virological and immunological responses to HAART Biomed Pharmacother 2005; 59: 446-51.]. The threshold of 200 CD4 cells/µL was taken as one decreasing the risk of serious opportunistic infections. However, the results were additionnally analyzed according to a threshold of CD4 > 400 cells/µL, which is one approaching normal values, and has been used in previous analyses of our cohort [19Jevtovic Dj, Salemovic D, Ranin J, Pešic I, Žerjav S, Djurkovic-Djakovic O. The dissociation between virological and immunological responses to HAART Biomed Pharmacother 2005; 59: 446-51.].
Laboratory Methods
CD4 cell counts and viral loads were measured in peripheral blood samples drawn at presentation and every 4-6 months during follow-up. CD4 cells were quantified by flow cytometry. Plasma HIV-1 RNA loads were measured by a quantitative reverse transcriptase polymerase chain reaction (Roche Molecular Systems, Branchburg, NY, USA), which has a lower limit of detection of 50 copies/mL (1.7 log10).
Statistics
All analyses were performed using an electronic database organized in the SPSS (version 11.5) statistical package. The association between the type of response to HAART, and variables including baseline and end-point CD4 cell counts and pVL, type of HAART regimen, and age above 40, were assessed using the chi-square test and univariate and multivariate logistic regression. Odds ratios (ORs) and the corresponding 95% confidence intervals (CIs) were used as estimators of relative risk for HAART failure, and/or lethal outcome. The Kaplan-Meier product limit method was used to determine the probability of reaching immunological and virological improvement, and survival, as well as to assess the probability of developing drug toxicities over time. One-way analysis of variance (ANOVA) was used to compare means. The level of statistical significance was 0.05.
RESULTS
Patient and Treatment Characteristics
Baseline characteristics of all patients are presented in Table 1.
Late presenters were more likely to be male (72.3%). Regarding transmission risk factors, the frequency of men having sex with men (MSM), heterosexuals and IV drug users was similar. There was only one patient who got infected vertically.
Treatment characteristics are presented in Table 2. The overall duration of HAART was 2.86 ± 1.80 years (range 1-9), but varied according to regimen. HAART regimens included combinations of two NRTIs as a treatment backbone, with (I) one or two PI (taken by 34.6% of all patients), (II) one NNRTI (35.6%), and (III) combinations of drugs from all three classes or triple NRTI regimens during some period of their treatment (29.7% switched multiple regimens during follow-up). Regimen sequencing was performed in case of virological and/or immunological failure, and also in some instances to simplify treatment by lowering pill burden. Antiretrovirals available in Serbia included zidovudine (AZT), lamivudine (3TC), didanosine (ddI), stavudine (d4T), abacavir (ABV), nevirapine, efavirenz, indinavir, saquinavir, nelfinavir, lopinavir/r, ritonavir(r), and enfuvirtide. Ritonavir was used for PI boosting only. Genotypic resistance testing was not routinely performed; thus, subsequent regimens were composed on the basis of standards of care [20Durant J, Clebenbergh P, Halfon P, et al. Drug-resistance genotyping in HIV-1 therapy: the VIRADEPT randomised controlled trial Lancet 1999; 353: 2195-9.]. However, three extensively pre-treated patients, after being diagnosed with multi drug-classes’ resistant virus, were switched to newer drugs, such as enfuvirtide, darunavir/r, and atazanavir/r (the latter two as a compassionate treatment).
TREATMENT EFFICACY
A favorable response to HAART was achieved in 55 (54.5%), a virological / immunological dissociation occurred in 32 (31.7%), while treatment failure was recorded in 14 (13.9%) patients (Table 3A). The mean number of drugs needed to achieve a favorable response was 4.8 ± 2.1 (range 3-10), similar (P > 0.05) to the number of drugs taken by those with HAART failure (5.0 ± 1.1) and a dissociative response (5.0 ± 1.5).
Gender, age over 40, and HIV transmission risk factor were not associated with HAART failure, nor was clinical AIDS at presentation (P > 0.05). Moreover, no specific AIDS-defining condition affected the type of response to HAART (P = 0.33), nor did any specific treatment regimen, whether PI- or NNRTI-based.
Ten (9.9%) patients died during the follow-up period. The most frequent causes of death were AIDS-related conditions including PML, TB, ADC, and disseminated CMV disease in two cases each, while non-Hodgkin lymphoma and end-stage HCV-related liver disease were the causes of death in one patient each. Of those with a fatal outcome, eight patients (80%) experienced HAART failure, and two (20%) had a dissociative response to HAART.
The overall estimated survival was eight years (Table 3B). Analysis of factors associated with survival showed that gender, age over 40, HIV disease stage, and HCV co-infection did not affect survival (P > 0.05), nor did specific AIDS-defining conditions. Survival was also unaffected by treatment regimen, whether PI- or NNRTI-based (P = 0.66). However, the achievement of undetectable viremia regardless of the degree of immune recovery was a predictor of longer survival (Figs. 1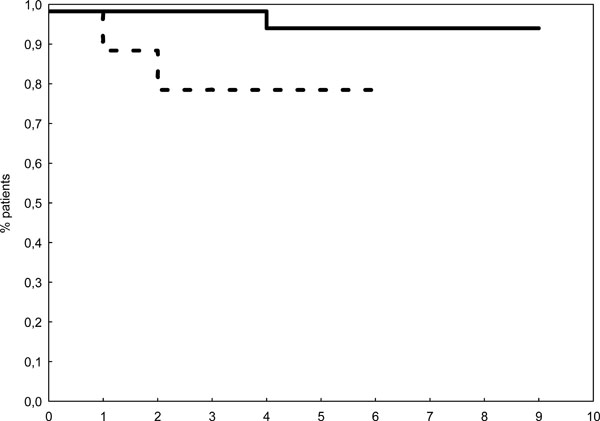 ,2
,2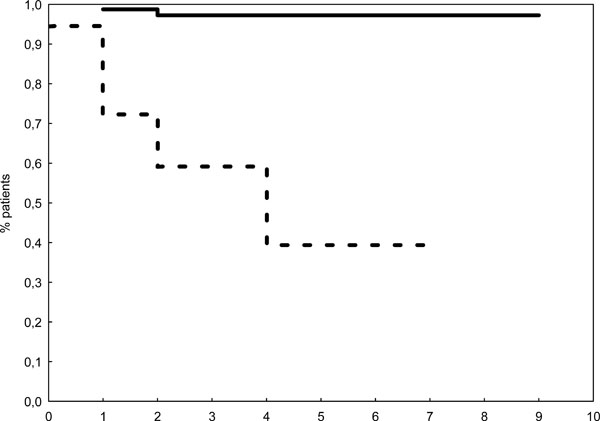 ). For patients with a mean viral load of 1.7 ± 0.23 (1.7 – 1.9), the estimated survival was 8.7 years, significantly longer (P < 0.001) than in those with a mean viral load of 3.6 ± 0.82 (2.9 – 5.2), whose estimated survival was 4.5 years. Achievement of undetectable viremia during treatment appeared life saving (OR = 42.5, 95% CI 7.1 – 251.9, P = 0.000), as was as a CD4 cell count of above 200/μL recorded in 57 (56.4%) patients (OR = 6.4, 95 CI 1.2-31.8, P = 0.023). The estimated survival in late presenters who achieved a rise in the CD4 cell count to above 200/μL was 8.7 years, as opposed to 5.8 years in those whose CD cell count did not recover to this level (P = 0.006) (Fig. 2). Interestingly, a CD4 count rise to over 400 cells/μL provided no extra benefit (P = 0.31, log rank). However, as revealed by multivariate logistic regression, achievement of undetectable viremia was the single independent predictor of survival (OR = 42.5, 95% CI 7.1 – 251.9, P = 0.000).
). For patients with a mean viral load of 1.7 ± 0.23 (1.7 – 1.9), the estimated survival was 8.7 years, significantly longer (P < 0.001) than in those with a mean viral load of 3.6 ± 0.82 (2.9 – 5.2), whose estimated survival was 4.5 years. Achievement of undetectable viremia during treatment appeared life saving (OR = 42.5, 95% CI 7.1 – 251.9, P = 0.000), as was as a CD4 cell count of above 200/μL recorded in 57 (56.4%) patients (OR = 6.4, 95 CI 1.2-31.8, P = 0.023). The estimated survival in late presenters who achieved a rise in the CD4 cell count to above 200/μL was 8.7 years, as opposed to 5.8 years in those whose CD cell count did not recover to this level (P = 0.006) (Fig. 2). Interestingly, a CD4 count rise to over 400 cells/μL provided no extra benefit (P = 0.31, log rank). However, as revealed by multivariate logistic regression, achievement of undetectable viremia was the single independent predictor of survival (OR = 42.5, 95% CI 7.1 – 251.9, P = 0.000).
 |
Fig. (1) Estimated probability of survival of late presenters according to achievement of undetectable viremia. pVL ≤ 2 log10 ___ , pVL ≥ 3log10 ----- , P = 0.009. |
 |
Fig. (2) Estimated probability of survival of late presenters according to achievement of CD4 cell coubt above 200/µL during HAART. Achieved ___ , not achieved ----- , P = 0.00. |
Immune restoration disease (IRD) developed in 11 (10.9%) patients, at a mean CD4 cell count of 270.4 ± 131.0. Dermatomal herpes zoster was the leading IRD manifestation, appearing in six patients. Other IRD presentations included CMV vitritis, genital herpes, TB, cryptococcal meningitis and a hepatitis flare in an HCV co-infected patient. The metabolic syndrome occurred frequently during treatment of late presenters. Hyper-lipidemia and lipodystrophy were recorded in 58 (7.4%) and 31 (30.6%) patients, respectively. Type 2 diabetes mellitus was recorded in 8 (7.9%). The median time to develop hyperlipidemia and lipodystrophy was 5 and 6 years, respectively. The 9-year probability of developing hyperlipidemia and lipodystrophy was 100%, while it was 30% for type 2 diabetes mellitus.
DISCUSSION
According to the results on the efficacy of HAART in our series of late presenters, these severely immunodeficient patients may have a rather good prognosis. Those who initiated HAART during or after recovering from opportunistic infections had a similar life expectancy as asymptomatic patients. Specific opportunistic events did not predict the outcome. If patients who commence HAART at a most advanced stage of HIV disease achieve undetectable viremia, they may have a very good prognosis even if the immune system has not recovered to the most desirable CD4 cell counts. Sabin et al. reported a 13% mortality among late presenters after a follow-up of 2.5 years [7Sabin CA, Smith CJ, Gumley H, et al. Late presenters in the era of highly active antiretroviral therapy: uptake of and response to antiretroviral therapy AIDS 2004; 18: 2145-51.]. If the results in our patient series are analyzed for this period, the mortality rate is quite similar (15.5%, data not shown). And moreover, since after a mean follow up of 2.9 ± 1.8 years the mortality rate dropped to 9.9%, HAART efficacy seems to increase over time. Hocking et al. suggested that increased survival of late presenters with AIDS on HAART may indicate a positive response of drug naive patients to antiretroviral therapies [6The Antiretroviral Therapy (ART) Cohort Collaboration. Prognosis of HIV-1 infected patients up to 5 years after initiation of HAART: collaborative analysis of prospective studies AIDS 2007; 21: 1185-97.].
Using the life expectancy model for the prognosis of HIV/AIDS in the HAART era, the ART Cohort Collaboration study reported a 8.5% mortality rate for patients who initiated HAART at a CD4 cell count below 50/µL [5The Antiretroviral Therapy Cohort Collaboration. Life expectance of individuals on combination antiretro-viral therapy in high-income countries: a collaborative analysis of 14 cohort studies Lancet 2008; 372: 393-9., 6The Antiretroviral Therapy (ART) Cohort Collaboration. Prognosis of HIV-1 infected patients up to 5 years after initiation of HAART: collaborative analysis of prospective studies AIDS 2007; 21: 1185-97.]. Even in the high income countries analyzed by the ART Cohort Collaboration study, late presentation had emerged as an issue of concern, since nearly one half of patients started HAART either with a CD4 cell count of less than 200 cells/ µL or with a diagnosis of AIDS. HIV management guidelines advocate early diagnosis and timely treatment. Such a strategy is essential to prevent clinical progression as well as the spread of the infection, in line with public health principles of wide screening and treatment shown to be effective in the control of many infectious diseases. The Centres for Disease Control and Prevention estimate that more than one half of new HIV infections are spread by HIV-positive individuals who are unaware of their infection, and thus support expanded, voluntary and cost-effective screening in healthcare settings, on the basis of opt-out strategy [21Advancing HIV prevention: new strategies for a changing epidemic - United States, 2003 MMWR 2003; 52: 329-.]. Wide voluntary screening in healthcare settings should be particularly advocated in Serbia, given that the HIV testing rate in Serbia is among the lowest in Europe.
Profound immunodeficiency on HAART initiation is associated with a risk of IRD. We, and others, have previously shown that a CD4 count below 100/µL at HAART initiation is a major risk factor for the development of IRD during HAART [22Jevtovic Dj, Salemovic D, Ranin J, Pesic I, Žerjav S, Djurkovic-Djakovic O. The incidence and risks for immune restoration disease in HAART-treated HIV patients treated with highly active antiretroviral therapy HIV Med 2005; 6: 140-3., 23Murdoch DM, Venter WDF, Van Rie A, Fildman C. Immune reconstitution inflammatory syndrome (IRIS): review of common infectious manifestations and treatment options AIDS Res Ther 2007; 4: 1-10.]. The overall prevalence of IRD among late presenters was 10.9 %, similar to our earlier data in the whole Serbian cohort of HIV/AIDS patients (16.7%) [22Jevtovic Dj, Salemovic D, Ranin J, Pesic I, Žerjav S, Djurkovic-Djakovic O. The incidence and risks for immune restoration disease in HAART-treated HIV patients treated with highly active antiretroviral therapy HIV Med 2005; 6: 140-3.]. IRD strongly affects the patients’ quality of life, since these episodes often require hospital admissions. Hyperlipidemia and lipodystrophy also emerged as important issues among late presenters on HAART, with an increased incidence as compared to the whole cohort [24Jevtovic Dj, Dragovic G, Salemovic D, Ranin J, Djurkovic Djakovic O. The metabolic syndrome, an epidemic among HIV infected patients on HAART Biomed Pharmacother 2009; 63: 337-42.].
Taken together, the presented results on HAART efficacy in late presenters indicate that reaching and maintaining undetectable viremia is a prerequisite for good prognosis for late presenters on HAART, regardless of the level of immune recovery.
ACKNOWLEDGEMENT
The work has been supported by grant M145002 from the Ministry of Science and Technological Development of Serbia.