- Home
- About Journals
-
Information for Authors/ReviewersEditorial Policies
Publication Fee
Publication Cycle - Process Flowchart
Online Manuscript Submission and Tracking System
Publishing Ethics and Rectitude
Authorship
Author Benefits
Reviewer Guidelines
Guest Editor Guidelines
Peer Review Workflow
Quick Track Option
Copyediting Services
Bentham Open Membership
Bentham Open Advisory Board
Archiving Policies
Fabricating and Stating False Information
Post Publication Discussions and Corrections
Editorial Management
Advertise With Us
Funding Agencies
Rate List
Kudos
General FAQs
Special Fee Waivers and Discounts
- Contact
- Help
- About Us
- Search


The Open Arthritis Journal
(Discontinued)
ISSN: 1876-5394 ― Volume 7, 2014
Peri-Arthritis and Tenosynovitis with a Ciprofloxacin-Resistant Gonococcal Strain
Freke Wink1, Filip Gemmel2, Henry de Vries3, Jan van Zeijl4 , George A.W. Bruyn*, 1
Abstract
Disseminated gonococcal infection (DGI) occurs in only a small minority of mucosal infections with Neisseria gonorrhoeae. Clinical manifestations of DGI include skin lesions, fever and musculoskeletal involvement. Articular manifestations include arthralgia, tenosynovitis, peri-arthritis and arthritis. Useful imaging techniques in DGI are multiphase bone scintigraphy and grey-scale ultrasonography with power Doppler modality. Sonography provides a reliable way to detect and aspirate fluid, which can be used for microbial diagnosis. Besides diagnostic purposes, cultivation allows determination of antimicrobial susceptibility, which may have implications for therapy. Since quinolone-resistant gonococcal infection continues to spread, treatment recommendations have changed to administration of cephalosporins in different parts of the world
Article Information
Identifiers and Pagination:
Year: 2009Volume: 2
First Page: 18
Last Page: 21
Publisher Id: TOARTHJ-2-18
DOI: 10.2174/1876539400902010018
Article History:
Received Date: 11/5/2009Revision Received Date: 8/7/2009
Acceptance Date: 18/7/2009
Electronic publication date: 1/10/2009
Collection year: 2009
open-access license: This is an open access article licensed under the terms of the Creative Commons Attribution Non-Commercial License (http: //creativecommons.org/licenses/by-nc/3.0/ which permits unrestricted, non-commercial use, distribution and reproduction in any medium, provided the work is properly cited.
* Address correspondence to this author at the Department of Rheumatology, Medisch Centrum Leeuwarden, 8934 AD Leeuwarden, The Netherlands; Tel: +31582866104; Fax: +31582866105; E-mail: gawbruyn@wxs.nl
| Open Peer Review Details | |||
|---|---|---|---|
| Manuscript submitted on 11-5-2009 |
Original Manuscript | Peri-Arthritis and Tenosynovitis with a Ciprofloxacin-Resistant Gonococcal Strain | |
INTRODUCTION
Systemic gonococcal manifestations result from the hematogenous spread of Neisseria gonorrhoeae usually from primary sexually acquired mucosal infection. Infrequently, direct invasion into the abdominal cavity may occur in infected female patients.
Due to effective control programmes the disease has become rare in Western countries, but gonococcal resistance to penicillin and tetracycline has been known for long time. Resistance to other antibiotics, particularly quinolones, has been reported to be on the rise in Asia and the Pacific. Several factors may account for this phenomenon. Sex tourism, mostly towards regions in Southeast Asia is popular and multi-resistant gonococci are increasingly cultured in patients from these regions [1-2]. In this report, we describe a typical presentation of disseminated gonococcal infection (DGI), with particular emphasis on imaging techniques and antibiotic resistance.
CASE REPORT
One week before admission to our hospital, a 50-year-old man presented at another hospital with a 10-day history of pain in the right ankle and right wrist, accompanied by erythema and swelling. Four weeks before admission, he had experienced fever and chills during a trip to Thailand and Indonesia. After a seafood dish, he had noted pustules on both the palms of his hands that disappeared shortly afterwards. In Thailand as well as in the Netherlands he had engaged in unprotected sex. There was no history of abdominal pain, diarrhea, dysuria or urethral discharge.
He had been on paracetamol and ibuprofen to alleviate the pain, but discontinued both drugs as it resorted little effect. There was a past history of nose polyps. There was no family history of rheumatic diseases or allergy.
On admission, blood pressure and pulse frequency were normal, temperature was 37.6 o C. Normal heart and lung sounds were noted. The abdomen was soft, with no signs of an enlarged liver or spleen. No lymphadenopathy was present. Swelling and erythema on the radial side of the right wrist as well as substantial swelling and erythema of the right ankle were present. The swelling and erythema extended upwards to halfway the medial side of the lower leg. Examination of the external genitalia was normal.
Laboratory screening showed erythrocyte sedimentation rate of more than 90 mm/hr, a C-reactive protein of 83 mg/L. White blood cell count was 13,5 × 109/L. Moreover, laboratory investigation showed mild elevation of liver function tests. Rheumatoid factor, antinuclear antibodies, anti-ds-DNA and antineutrophil cytoplasmatic antibodies were all negative. Roentgenograms of right knee and right ankle both showed soft tissue swelling without erosions or bone lesions. A chest radiograph was normal. A two-phase bone scintigraphy with Technetium-999 HDP (Tc-HDP) showed a superficial linear hyperaemia at the right wrist, diffuse hyperaemia both at the medial right ankle and at the right knee region. Delayed static images, 3 hours post-injection, revealed a marked bony uptake at the medial side of the right ankle, a mild focal bony uptake in the radial styloïd and a diffuse infiltration of the soft tissues in the right leg (Fig. 1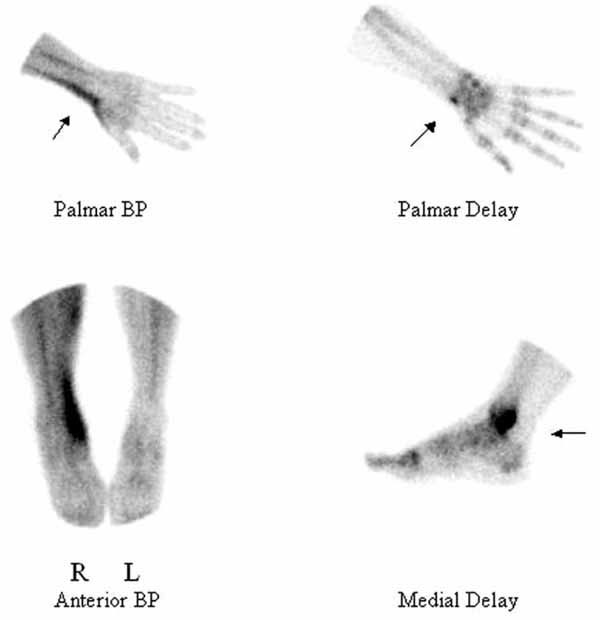 ).
).

Sonography of the right ankle revealed fluid and synovial thickening around the tendon of the tibialis posterior muscle (Fig. 2A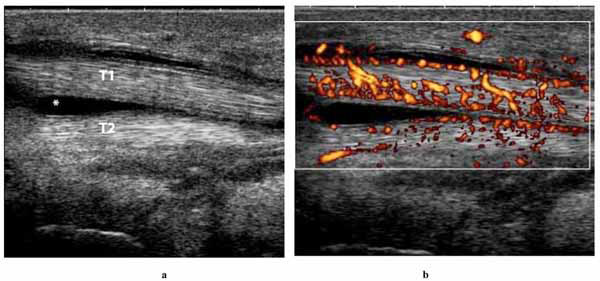 ). On power Doppler imaging there was increased blood flow around this tendon, compatible with inflammation (Fig. 2B). About 5 mL of turbid fluid, orange-brown in appearance, was sonographically-guided aspirated from the fluid collection within the sheath of the tibialis posterior tendon.
). On power Doppler imaging there was increased blood flow around this tendon, compatible with inflammation (Fig. 2B). About 5 mL of turbid fluid, orange-brown in appearance, was sonographically-guided aspirated from the fluid collection within the sheath of the tibialis posterior tendon.

Polarisation microscopic examination of a wet-mount preparation of the fluid showed no crystals, but a direct Gram stain of the aspirate showed intracellular gram-negative microorganisms (Fig. 3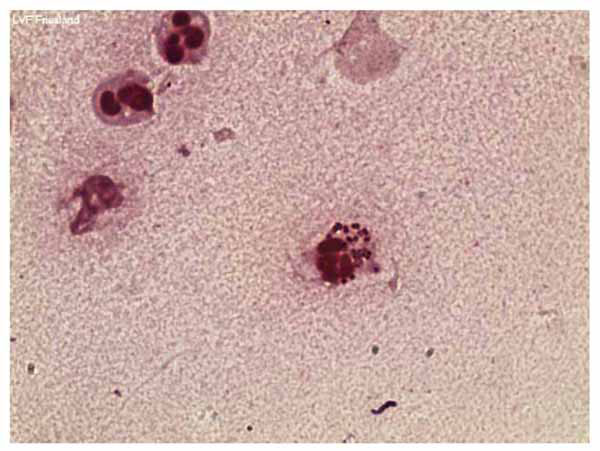 ). Culture of the aspirate grew betalactamase-producing and ciprofloxacin resistant N. gonorrhoeae. Nucleic acid amplified tests on a urethral swab for N.gonorrhoeae and Chlamydia trachomatis were negative, as well as serologic screening for syphilis and HIV antibodies.
). Culture of the aspirate grew betalactamase-producing and ciprofloxacin resistant N. gonorrhoeae. Nucleic acid amplified tests on a urethral swab for N.gonorrhoeae and Chlamydia trachomatis were negative, as well as serologic screening for syphilis and HIV antibodies.
 |
Fig. (3) Gram stain of tenosynovial fluid showing intra- and extracellular gonococci. |
Treatment consisted of two weeks parenteral administration of one gram ceftriaxone twice daily, resulting in disappearance of all musculoskeletal manifestations and normalisation of inflammatory parameters.
DISCUSSION
In this report we present a patient with a peri-arthritis of the right wrist and ankle due to tenosynovitis as first manifestations of a systemic gonococcal infection. Recognized features of systemic gonococcal infection are asymmetric oligoarthritis, skin rash and fever. Frank arthritis develops in less than 50 % of patients with DGI. Arthritic involvement is typically oligoarticular, asymmetrical, and most frequently involves knees, wrists and ankles [3]. In addition, periarticular symptoms, as in our case, have been described [3-4]. Tenosynovitis is one of the most characteristic features of DGI . Most often it affects multiple tendons simultaneously, particularly those of the wrist, ankle, fingers and toes. It may occur in up to 50-60 % of patients with DGI, with or without joint involvement.
In the USA, gonorrhea is the second most commonly reported notifiable disease [5]. The estimated national prevalence of gonococcal infection among persons 14-39 years of age is 0.25% [6]. Infection with N. gonorrhoeae, a gram-negative diplococcus, has a mean incubation period of 2-7 days, with a spread from 2 to 14 days. Gonococcal infections in men may involve any part of the urogenital tract, leading to dysuria, mucopurulent urethral discharge or epididymitis. In women, gonorrhea often follows an asymptomatic course, but may result in vaginal fluor complaints, pelvic inflammatory disease (PID) or infertility. Dissemination occurs in 0.5-3 % of the infected patients [7]. As in this case, disease may result from asymptomatic carriership of N. gonorrhoeae.
Advanced imaging techniques including grey-scale and power Doppler sonography and bone scintigraphy are able to exhibit the full extent of the disease and to establish the diagnosis. Three or two-phase bone scintigraphy is a very useful non-invasive imaging modality for early detection of various soft-tissue and osseous pathologies [8]. Moreover, the whole body scanning capability is an advantage compared to other radiological modalities.
The scintigraphic pattern of remarkable focal blood pool activity or hyperaemia but without articular involvement is most compatible with soft tissue inflammation, such as a tendonitis or tenosynovitis. Tenosynovitis can be best detected in the first phases of the bone scintigraphy, i.e., within the first 5 minutes after the intravenous injection of the Tc-labeled bone-imaging agent. Furthermore, the sometimes subtle diphosphonate uptake can be missed on delayed images when no additional detailed views are made [9]. In addition, it may show a cellulitis, as in our patient.
The role of bone scintigraphy in the detection of infectious tenosynovitis is rarely reported in the literature, mainly as case reports [9]. Hung et al. described a young woman with systemic lupus erythematosus who developed an infection with Mycobacterium avium complex tenosynovitis of the right index finger, illustrated by 3-phase bone scan [10]. Abdelwahab et al. reported recently on tuberculous tenosynovitis involving the hand/wrist and ankle/foot with bone scan and other imaging modalities [11]. However, bone scanning is not specific enough in discriminating infectious from inflammatory tenosynovitis. To establish a definite diagnosis, more invasive tests are needed.
Over the last few years, grey-scale ultrasonography has emerged as a powerful tool to detect effusions and synovitis in joints and tendon sheaths as well as other soft tissue pathology. Colour and power Doppler ultrasonography (PDUS) are both able to detect synovial blood flow movement [12]. Most modern US machines offer the option to use either colour or power Doppler mode. When using modern US equipment, the sensitivity of PDUS is probably similar to the sensitivity of colour Doppler for small-vessel imaging. The increased blood flow around the tibialis posterior tendon shown by PDUS illustrates the intense inflammation that accompanied the gonococcal infection. The combined use of grey-scale ultrasonography and PDUS provided additional information about the location and extent of inflammatory hyperemia. We used grey-scale ultrasonography to assess for fluid collections, with the additional advantage to target aspiration of fluid for diagnostic culture. Because of the diffuse swelling and erythema of the ankle and lower leg, aspiration of fluid would have been much more difficult without the use of these imaging modalities.
For establishing a definite diagnosis and determination of antimicrobial susceptibility, the isolation of N. gonorrhoeae is required. The gonococcal strain isolated from our patient was resistant to quinolones. In 2002, the Centers for Disease Control in the United States advised that quinolones should not longer be used in certain states, including California and Hawaii, because of the high prevalence of quinolone-resistance [13-14]. In the Netherlands, the resistance of gonococci to quinolones rapidly increased, from 7 % in 2002 to 26 % in 2005 [15]. Since resistance to quinolones in Southeast Asia contributes to the spread of these strains in Europe, the Netherlands Society for Dermatology and Venereology has changed its treatment advice for gonococcal infection in 2004 to the intramuscular administration of ceftriaxone or cefotaxim. Ceftriaxone in a single injection of 125 milligram provides a high bactericidal blood level. Extensive evidence has shown that ceftriaxone is a safe and efficacious treatment for uncomplicated gonococcal infection at all anatomical sites, curing almost 99 % of infections [16].
Crucial for guiding in local therapy recommendations is surveillance for antimicrobial susceptibility of N. gonorrhoeae strains. In the Netherlands the increase in quinolone-resistant gonococci has resulted in a new surveillance program in which all positive cultures for N. gonorrhoeae will be investigated on antimicrobial susceptibility and epidemiological features.