- Home
- About Journals
-
Information for Authors/ReviewersEditorial Policies
Publication Fee
Publication Cycle - Process Flowchart
Online Manuscript Submission and Tracking System
Publishing Ethics and Rectitude
Authorship
Author Benefits
Reviewer Guidelines
Guest Editor Guidelines
Peer Review Workflow
Quick Track Option
Copyediting Services
Bentham Open Membership
Bentham Open Advisory Board
Archiving Policies
Fabricating and Stating False Information
Post Publication Discussions and Corrections
Editorial Management
Advertise With Us
Funding Agencies
Rate List
Kudos
General FAQs
Special Fee Waivers and Discounts
- Contact
- Help
- About Us
- Search




The Open Virology Journal
(Discontinued)
ISSN: 1874-3579 ― Volume 15, 2021
Therapeutic Human Papillomavirus (HPV) Vaccines: A Novel Approach
Kei Kawana*, Katsuyuki Adachi, Satoko Kojima, Shiro Kozuma, Tomoyuki Fujii
Abstract
Cervical cancer is the second largest cause of cancer-related death in women worldwide, and it occurs following persistent infection, sometimes for decades, with a specific subset of human papillomavirus (HPV) types; the approximately 13 oncogenic subtypes. Prophylactic vaccines against HPV infections hold promise for cost-effective reductions in the incidence of cervical cancer, but this may not be enough. Two prophylactic HPV vaccines are presently available and both contain L1 virus-like particles (VLPs) derived from the HPV subtypes most frequently associated with cervical cancer, HPV-16 and -18. Since the L1-VLP vaccines can only effectively prevent infection by the specific HPV subtype against which the vaccine was developed, cervical cancers caused by high-risk HPV subtypes other than HPV-16 and -18 may still occur in recipients of the current HPV vaccines. Furthermore, HPV vaccination coverage for adolescents is insufficient in most countries and therefore even HPV-16 and -18 infections are unlikely to be fully eradicated using the existing strategies. The development of HPV therapeutic vaccines remains essential. Many therapeutic vaccines aimed at clearing HPV-related cervical lesions have been developed and tested in patients with HPV16-positive cervical intraepithelial lesions (CIN) or cervical cancers. To date, definitive clinical efficacy and appropriate immunological responses have never been demonstrated for cervical neoplasia although promising results have been reported in patients with vulvar intraepithelial neoplasia. Here we discuss shortcomings of previous HPV therapeutic vaccine candidates and propose a novel vaccination strategy that leverages newly gained knowledge about mucosal immunity and the induction of mucosal immune responses.
Article Information
Identifiers and Pagination:
Year: 2012Volume: 6
Issue: Suppl 2
First Page: 264
Last Page: 269
Publisher Id: TOVJ-6-264
DOI: 10.2174/1874357901206010264
Article History:
Received Date: 16/2/2012Revision Received Date: 28/7/2012
Acceptance Date: 10/8/2012
Electronic publication date: 28/12/2012
Collection year: 2012
open-access license: This is an open access article licensed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted, non-commercial use, distribution and reproduction in any medium, provided the work is properly cited.
* Address correspondence to this author at the Department of Obstetrics and Gynecology, Faculty of Medicine, University of Tokyo, 7-3-1 Hongo, Bunkyo-ku, Tokyo 113-8655, Japan; Tel: 81-3-3815-5411; Fax: 81-3-3816-2017; E-mail: kkawana-tky@umin.org
| Open Peer Review Details | |||
|---|---|---|---|
| Manuscript submitted on 16-2-2012 |
Original Manuscript | Therapeutic Human Papillomavirus (HPV) Vaccines: A Novel Approach | |
EPIDEMIOLOGY OF HPV INFECTION
At present, there are about 100 identified genotypes (types) of human papillomavirus (HPV) of which about 40 are genital HPV types that invade genital organs such as the uterine cervix, vaginal wall, vulva, and penis. Genital HPV types are classified into high-risk types commonly associated with cervical cancer and low-risk types known to cause condyloma acuminatum. This classification varies among researchers, but, in general, types 16/18/31/33/35/39/45/51/52/56/58/66/68 are classified as high-risk and 6/11/40/42/43/ 44/54/61/72 as low-risk [1 zur Hausen H. Papillomavirus and cancer: from basic studies to
clinical application Nat Rev Cancer 2002; 2: 342-50.]. Interestingly, the HPV type distribution varies depending on the stage of cervical neoplasia (Fig. 1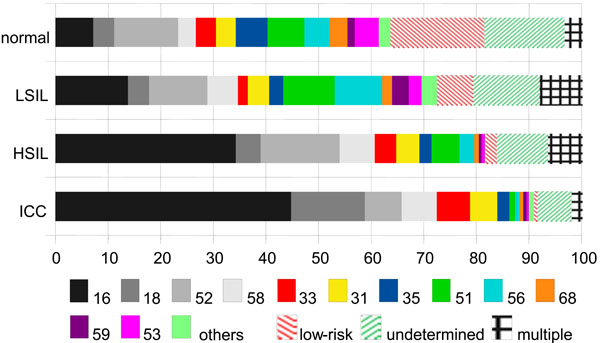 ).
).
 |
Fig. (1) HPV subtype distribution in cervical neoplastic lesions in Japan [18 Ochi H, Kondo K, Matsumoto K, et al. Neutralizing antibodies against human papillomavirus types 16, 18, 31, 52, and 58 in serum samples from women in Japan with low-grade cervical intraepithelial neoplasia Clin Vaccine Immunol 2008; 15: 1536-40.]. HPV16 and 18 are the most common subtypes found in invasive cervical cancer (ICC) but more than 40% of invasive lesions are associated with other oncogenic subtypes in Japan. HPV52 is the most common HPV subtype present among Japanese women with with normal cervical cytology [19 Villa LL, Costa RL, Petta CA, et al. High sustained efficacy of a prophylactic quadrivalent human papillomavirus types 6/11/16/18 L1 virus-like particle vaccine through 5 years of follow-up Br J Cancer 2006; 95: 1459-66.]. |
The HPV DNA detection rate in the genital organs of healthy adult females varies between advanced and developing countries but is approximately 20-40% collectively [2 Dunne EF, Unger ER, Sternberg M, et al. Prevalence of HPV infection among females in the United States JAMA 2007; 297: 813-9., 3 Bosch FX, de Sanjose S. Human papillomavirus and cervical cancer – burden and assessment of causality J Natl Cancer Inst Monogr 2003; 31: 3-13.]. In Japan, the HPV-positive rate in pregnant females aged 20-29 years has been reported to be 20-30%, which is similar to or higher than that among similarly aged females in the U.S [4 Masumoto N, Fujii T, Ishikawa M, et al. Dominant human papillomavirus 16 infection in cervical neoplasia in young Japanese women, study of 881 outpatients Gynecol Oncol 2004; 94: 509-14.]. The World Health Organization (WHO) has estimated an annual increase of 3 hundred million in the number of HPV carriers in the world [5 The current status of development of prophylactic vaccines against human papillomavirus infection Report of a technical meeting 16- 18 February 1999; Geneva , 6 Ho GY, Bierman R, Beardsley L, Chang CJ, Burk RD. Natural history of cervicovaginal papillomavirus infection in young women N Engl J Med 1998; 338: 423-8.]. Overall HPV prevalence with normal cervical cytology was estimated to be 10.4 % [6 Ho GY, Bierman R, Beardsley L, Chang CJ, Burk RD. Natural history of cervicovaginal papillomavirus infection in young women N Engl J Med 1998; 338: 423-8.]. Epidemiological data show HPV infection at least once during their lifespan in approximately 75 % of U.S. women [3 Bosch FX, de Sanjose S. Human papillomavirus and cervical cancer – burden and assessment of causality J Natl Cancer Inst Monogr 2003; 31: 3-13.]. Thus, HPV infection is common and can affect any female. Frequent sexual activity has been reported to increase the risk of HPV infection but this is not always the case [7 de Sanjosé S, Diaz M, Castellsagué X, et al. Worldwide prevalence and genotype distribution of cervical human papillomavirus DNA in women with normal cytology: a meta-analysis Lancet Infect Dis 2007; 7: 453-9.].
NATURAL HISTORY OF CERVICAL INTRAEPITHELIAL NEOPLASIA
Natural history studies of CIN show that most infections and CIN lesions resolve spontaneously but some persist and progress to cervical cancer. The incidence of cervical intraepithelial neoplasia (corresponding to squamous intraepithelial lesion: SIL) is about 1 per 10 females with HPV infection [8 Koutsky L. Epidemiology of genital human papillomavirus infection Am J Med 1997; 102: 3-8.]. The incidence of high grade SIL (corresponding to cervical intraepithelial neoplasia 2 and 3: CIN2-3) is about 3 per 10 females with low grade SIL, and that of CIN3 is about 1-2 per 10 females with low grade SIL [9 Trottier H, Franco EL. The epidemiology of genital human papillomavirus infection Vaccine 2006; 24S1: S1/4-S1/15.]. Without treatment, the incidence of the progression of CIN3 to cervical cancer is about 30% [10 Holowaty P, Miller AB, Rohan T, To T. Natural history of dysplasia of the uterine cervix J Natl Cancer Inst 1999; 91: 252-8.]. Therefore, the incidence of the spontaneous development of cervical cancer is about 1 per 200-300 females with HPV infection. Factors associated with progression to cervical cancer in females with HPV infection have been extensively studied [1 zur Hausen H. Papillomavirus and cancer: from basic studies to clinical application Nat Rev Cancer 2002; 2: 342-50.]. Many prospective studies have identified persistent HPV infection as the most important risk factor. They have also shown that persistent infection tends to occur in women with high risk HPV subtypes.
Chronic virus proliferation induces the active proliferation/differentiation of infected epithelial cells, and some infected cells incidentally immortalize, which is the first step of carcinogenesis [1 zur Hausen H. Papillomavirus and cancer: from basic studies to clinical application Nat Rev Cancer 2002; 2: 342-50.]. In contrast, transient infection involves short-term virus proliferation followed by the long-term latent presence of low copies of the viral genome in the basal cells of the genital epithelium [11 Gravitt PE. The known unknows of HPV natural history J Clin Invest 2011; 121: 4593-9.]. Studies showing that HIV-infected women and patients who are under treatment with immunosuppressive agents have an increased incidence of CIN lesions [12 Ellerbrock TV, Chiasson MA, Bush TJ, et al. Incidence of cervical squamous intraepithelial lesions in HIV-infected women JAMA 2000; 283: 1031-7., 13 Ognenovski VM, Marder W, Somers EC, et al. Increased incidence of cervical intraepithelial neoplasia in women with systemic lupus erythematosus treated with intravenous cyclophosphamide J Rheumatol 2004; 31: 1763-7.] suggest that cell-mediated immune response against HPV antigens is important in the control of HPV infection and progression to CIN. More controversial are the relative roles of systemic and local mucosal immune responses in HPV pathogenesis [14 Kawana K, Yasugi T, Taketani Y. Human papillomavirus vaccines: current issues and future: Review Indian J Med Res 2009; 130: 341-7.]. Trimble et al. reported that naturally occurring systemic immune responses to HPV antigens do not predict regression of CIN 2/3 lesions [15 Trimble CL, Peng S, Thoburn C, Kos F, Wu TC. Naturally occurring systemic immune responses to HPV antigens do not predict regression of CIN2/3 Cancer Immunol Immunother 2010; 59: 799-803.] but Nakagawa et al. demonstrated a positive association between systemic cell-mediated immune responses to HPV E6 and the regression of HPV/CIN [16 Nakagawa M, Gupta SK, Coleman HN, Sellers MA, Banken JA, Greenfield WW. A favorable clinical trend is associated with CD8 T-cell immune responses to the human papillomavirus type 16 E6 antigens in women being studied for abnormal pap smear results J Low Genit Tract Dis 2010; 14: 124-9.].
SHORTCOMINGS OF THE CURRENT L1-VLP VACCINES
Theoretically, if HPV infection could be completely eradicated, HPV-associated cancers could be prevented. With this in mind, HPV vaccines began to be studied nearly 10 years ago. In 2002, Koutsky et al. were the first to show the clinical prophylactic effects of an HPV vaccine [17 Koutsky LA, Ault KA, Wheeler CM, et al. A controlled trial of a human papillomavirus type 16 vaccine N Engl J Med 2002; 347: 1645-51.]. Soon thereafter, Merck in the United States and Glaxo Smith Kline (GSK) in Europe launched full-scale development of prophylactic vaccines against HPV. These products were approved and became commercially available just a few years ago. The vaccine antigens used by the two companies are virus-like particles (VLP) produced by overexpressing HPV16 L1 protein in yeast or insect cells. These particles have a 3-dimensional external structure similar to that of virus particles, but having no internal contents, they are not infective. The vaccine first reported by Koutsky et al. also used HPV16L1-VLP as an antigen.
One integral drawback of L1-VLP based vaccines is their negligible prophylactic effect on many HPV subtypes not specifically targeted by the vaccine [18 Ochi H, Kondo K, Matsumoto K, et al. Neutralizing antibodies against human papillomavirus types 16, 18, 31, 52, and 58 in serum samples from women in Japan with low-grade cervical intraepithelial neoplasia Clin Vaccine Immunol 2008; 15: 1536-40.]. For this reason, GSK and Merck developed cocktail vaccines composed of L1-VLPs corresponding to several HPV subtypes. The vaccine developed by Merck is a quadrivalent vaccine against HPV types 6, 11, 16, and 18 (Gardasil®) [19 Villa LL, Costa RL, Petta CA, et al. High sustained efficacy of a prophylactic quadrivalent human papillomavirus types 6/11/16/18 L1 virus-like particle vaccine through 5 years of follow-up Br J Cancer 2006; 95: 1459-66.] and that developed by GSK is a bivalent vaccine against types 16 and 18 (Cervarix®) [20 Harper DM, Franco EL, Wheeler CM, Moscicki AB, et al. Sustained efficacy up to 4??5 years of a bivalent L1 virus-like particle vaccine against human papillomavirus types 16 and 18: follow-up from a randomised control trial Lancet 2006; 367: 1247-55.]. Unfortunately these L1-VLP vaccines are very specific and may not protect for long time against HPV types that exhibit very close genetic similarities to HPV-16 or -18, such as HPV-58 or -45 respectively. Ultimately, the most effective L1-VLP-based vaccines vaccines would be multivalent for the 13 described oncogenic HPV types. Such prophylactic vaccines would likely be much more expensive than their current counterparts.
HPV-16 or -18-related cervical cancers, which constitute less than 60% of all invasive cervical cancer cases in Japan [21 Miura S, Matsumoto K, Oki A, et al. Do we need a different
strategy for HPV screening and vaccination in East Asia? Int J
Cancer 2006; 119: 2713-5.], could be prevented if the appropriate subtype cocktail vaccine were available (Fig. 1). However, the HPV subtype distribution in cervical cancer varies (60-70%) by worldwide location [22 Clifford GM, Smith JS, Plummer M, Muñoz N, Franceschi S.
Human papillomavirus types in invasive cervical cancer
worldwide: a meta-analysis Br J Cancer 2003; 88: 63-73.] and current vaccines are unable to address all oncogenic subtypes in even a single population. While current HPV vaccines are distributed without cost to the patient due to government subsidies or full coverage by insurance [23Wright TC Jr. Current status of HPV vaccination recommendation
HPV Today 2008; 14: 8-9.] these facile approaches will ultimately fail to eradicate the disease. Further, even with broad vaccination coverage, deficiencies in vaccine design mandate that even vaccinated females must continue cervical cancer screening.
The commercially available GSK and Merck HPV vaccines are indicated for uninfected females to prevent HPV infection/spread. Due to the high prevalence of HPV infection, effective mass prophylactic vaccination strategies for uninfected females should include girls age 10 and above to predate the onset of sexual activity. Ph-III clinical studies in which females approximately 20 years of age were randomly inoculated with Gardasil® or Cervarix® revealed protective efficacy on the development of CIN2-3 associated with HPV-16 or -18 in 93-98% of vaccine-type naïve females who completed the vaccination protocol [24 Muñoz N, Kjaer SK, Sigurdsson K, et al. Impact of Human papillomavirus (HPV)-6/11/16/18 vaccine on all HPV-associated genital diseases in young women J Natl Cancer Inst 2010; 102: 25-39., 25 Paavonen J, Naud P, Salmerón J, et al. Efficacy of human papillomavirus (HPV)-16/18 AS04-adjuvanted vaccine against cervical infection and precancer caused by oncogenic HPV types (PATRICIA): Final analysis of a double-blind, randomised study in young women Lancet 2009; 374: 301-14.]. However, intention-to-treat analysis revealed protective efficacy was only 19-30% for non-vaccine HPV subtypes [24 Muñoz N, Kjaer SK, Sigurdsson K, et al. Impact of Human papillomavirus (HPV)-6/11/16/18 vaccine on all HPV-associated genital diseases in young women J Natl Cancer Inst 2010; 102: 25-39., 25 Paavonen J, Naud P, Salmerón J, et al. Efficacy of human papillomavirus (HPV)-16/18 AS04-adjuvanted vaccine against cervical infection and precancer caused by oncogenic HPV types (PATRICIA): Final analysis of a double-blind, randomised study in young women Lancet 2009; 374: 301-14.].
DEVELOPMENT OF HPV THERAPEUTIC VACCINES
The limitations of current prophylactic HPV vaccines demonstrate a pressing need for novel approaches to the eradication of HPV-related neoplasia and suggest that the development of therapeutic vaccines for the treatment of HPV-associated lesions will remain an important goal even if worldwide prophylactic vaccine programs are successfully implemented [26 Kanodia S, Da Silva DM, Kast WM. Recent advances in strategies for immunotherapy of human papillomavirus-induced lesions Int J Cancer 2008; 122: 247-59.]. The past two decades has seen several inroads into the development of therapeutic HPV vaccines. The combined actions of the high-risk E6 and E7 oncoproteins are essential for the maintenance of the neoplastic phenotype and the evasion of apoptosis. Several functions have been described for E6 and E7. Initial observations revealed that E6 interacts with p53 and E7 interacts with Rb to block the activity of these tumour suppressors [1 zur Hausen H. Papillomavirus and cancer: from basic studies to clinical application Nat Rev Cancer 2002; 2: 342-50.]. There are only two possible antigenic targets, E6 and E7, since these are the only viral proteins that will be expressed in all cancers and precursor lesions [1 zur Hausen H. Papillomavirus and cancer: from basic studies to clinical application Nat Rev Cancer 2002; 2: 342-50.]. The approach of deliberate immunization with E6 and/or E7 of HPV 16 and 18 predominantly, and the generation of antigen-specific CTL as an immunotherapy for HPVassociated cancer has been tested with a wide array of potential vaccine delivery systems. Here we will summarize the results of the therapeutic vaccine clinical trials reported to (Table 1) [14 Kawana K, Yasugi T, Taketani Y. Human papillomavirus vaccines: current issues and future: Review Indian J Med Res 2009; 130: 341-7.].
- SGN-00101 (s.c.) is a fusion protein consisting of a heat shock protein (Hsp) from Mycobacterium bovis and HPV16 E7. The Ph-II study looking at the effects of SGN-00101 in women with CIN3 revealed histological regression to CIN1or less (complete remission: CR) in 13 (22.5%) of 58 cases, although immunological responses were not studied [27 Einstein MH, Kadish AS, Burk RD, et al. Heat shock fusion protein-based immunotherapy for treatment of cervical intraepithelial neoplasia III Gynecol Oncol 2007; 106: 453-60.]. Another Ph-II study of the same agent administered to women with CIN showed the induction of cytotoxic T lymphocyte (CTL) against HPV16E7 in peripheral monocytes in 5 of 7 patients which obtained CR [28 Roman LD, Wilczynski S, Muderspach LI, et al. A phase II study of Hsp-7 (SGN-00101) in women with high-grade cervical intraepithelial neoplasia Gynecol Oncol 2007; 106: 558-66.].
- L1VLP-E7 (s.c.) is a vaccine using chimeric particles composed of HPV16 L1-VLP and E7. In the Ph-I/II study of women with CIN2-3, histological regression to CIN2 (partial remission; PR) was shown in 39% of vaccine recipients compared with 25 % of placebo recipients. This was not significant significant [29 Kaufmann AM, Nieland JD, Jochmus I, et al. Vaccination trial with HPV16 L1E7 chimeric virus-like particles in women suffering from high grade cervical intraepithelial neoplasia (CIN 2/3 Int J Cancer 2007; 121: 2794-800.]. Clinical response was coupled with detectable cellular immune responses in some cases.
- TA-HPV (i.m.) is a recombinant vaccinia virus expressing E6 and E7 of HPV-16 and -18. The Ph-II study of TA-HPV in women with vulvar intraepithelial neoplasia (VIN) revealed PR of lesions in 8 of 13 cases and responders also had an increase in lesion-infiltrating CD4 and CD8 positive cells [30 Davidson EJ, Boswell CM, Sehr P, et al. Immunological and clinical responses in women with vulval intraepithelial neoplasia vaccinated with a vaccinia virus encoding human papillomavirus 16/18 oncoproteins Cancer Res 2003; 63: 6032-41.].
- TA-CIN (i.m.) is a fusion protein consisting of E6, E7 and L2 from HPV-16 and -18. The Ph-II study in women with VIN revealed CR or PR in only 6 of 29 cases. CTL against E6/E7 were induced in 4 of 29 cases [31 Fiander AN, Tristram AJ, Davidson EJ, et al. Prime-boost vaccination strategy in women with high-grade, noncervical anogenital intraepithelial neoplasia: clinical results from a multicenter phase II trial Int J Gynecol Cancer 2006; 16: 1075-81.]. Correlations between clinical efficacy and cellular immune responses to the vaccine remain unclear.
- MVA-E2 (TGA4001) (intrauterine) is also a recombinant vaccinia virus expressing bovine papilloma virus (BPV) E2. A Ph-II study in subjects with CIN2-3 confirmed the down grade of CIN in some cases (19/34 cases) [32 García-Hernández E, González-Sánchez JL, Andrade-Manzano A, et al. Regression of papilloma high-grade lesions (CIN 2 and CIN 3) is stimulated by therapeutic vaccination with MVA E2 recombinant vaccine Cancer Gene Ther 2006; 13: 592-7.].
- ZYC-101a (i.m.) is a DNA vaccine synthesized from proteins containing CTL epitopes against E6 and E7 of HPV-16 and -18. A Ph-III study was performed in subjects with CIN2-3. CR or PR was observed in 41% of vaccinated women and 27% of those receiving placebo. This was not a significant difference. Subset-analysis limited to those subjects aged 25 years or less revealed a statistically significant increase in the percentage of women with CR or PR in the vaccination group (72%) when compared to placebo controls (23%). However, no correlation was shown between CTL induction against E6/E7 and clinical effect [33 Garcia F, Petry KU, Muderspach L, et al. ZYC101a for treatment of high-grade cervical intraepithelial neoplasia: a randomized controlled trial Obstet Gynecol 2004; 103: 317-26.].
- Synthetic long-peptide vaccine (s.c.) is a peptide vaccine comprised of nine HPV16 E6 peptides and four HPV16 E7 peptides solubilized in incomplete Freund’s adjuvant. A Ph-II study was performed in patients with VIN3. 5 of 20 patients demonstrated complete regression of their lesions [34 Kenter GG, Welters MJ, Valentijn AR, et al. Vaccination against HPV-16 oncoproteins for vulvar intraepithelial neoplasia N Engl J Med 2009; 361: 1838-47.].
In summary, no therapeutic HPV vaccines are presently available that exert significant clinical efficacy against CIN. Some of the tested therapeutic vaccines elicited systemic cellular immunity after intramuscular or subcutaneous injection, but none of the trials have assessed local cellular immune responses to vaccine antigen in the cervix.. The outcomes of vaccination strategies involving intramuscular or subcutaneous injection of E6/E7-based antigens for the treatment of VIN have been more promising [30 Davidson EJ, Boswell CM, Sehr P, et al. Immunological and clinical responses in women with vulval intraepithelial neoplasia vaccinated with a vaccinia virus encoding human papillomavirus 16/18 oncoproteins Cancer Res 2003; 63: 6032-41., 31 Fiander AN, Tristram AJ, Davidson EJ, et al. Prime-boost vaccination strategy in women with high-grade, noncervical anogenital intraepithelial neoplasia: clinical results from a multicenter phase II trial Int J Gynecol Cancer 2006; 16: 1075-81., 34 Kenter GG, Welters MJ, Valentijn AR, et al. Vaccination against HPV-16 oncoproteins for vulvar intraepithelial neoplasia N Engl J Med 2009; 361: 1838-47.]. We hypothesize that these findings are the direct result of the predicted poor response of cervical mucosal lesions to systemic cellular immune responses when compared to the effects of systemic immunity on epidermal lesions including those of VIN.
THE CERVICAL MUCOSAL IMMUNE SYSTEM AND HPV THERAPEUTIC VACCINES
Induction of adaptive cellular immune responses to HPV in the cervical mucosa is indispensable for treating cervical mucosal lesions such as CIN. Since precancerous lesion of the cervix develops essentially exclusively in the mucosal epithelium it would be predicted that intraepithelial lymphocytes (IELs) should be central to the elimination of CIN. To this poin, there are substantial differences between cellular and humoral immune responses in the female reproductive tract mucosa. It is well-known that intramuscular injection of L1-VLP based vaccines leads to systemic humoral immune responses characterized by the induction of anti-L1 IgG neutralizing antibody which leaks from the serum to protect the reproductive tract mucosa from HPV infection. However, the requirements for induction of mucosal cellular immune responses against microbial infected lesions differ from and are independent of those for systemic cellular immunity. Therefore, systemic intramuscular or subcutaneous vaccination strategies may be unsuitable for the induction of mucosal cellular immunity, at least in the reproductive tract mucosa.
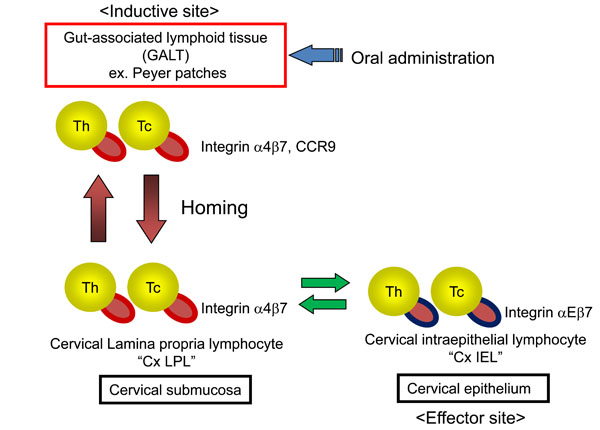
In the uninduced state, the specific lymphocytes involved in mucosal immunity reside in the inductive sites of organized mucosa-associated lymphoid tissues (MALT); these are present in a variety of effector sites, including the mucosa of the intestine, respiratory tract and genital tract [35 Gorfu G, Nieves JR, Ley K. Role of beta7 integrins in intestinal
lymphocyte homing and retention Curr Mol Med 2009; 9: 836-50.]. Efficient homing of lymphocytes to the gut is dependent on the homing receptors integrin α4β7 and C-C chemokine receptor type 9 (CCR9). Lymphocyte-expressed integrin α4β7 and CCR9 bind to their natural ligands, mucosal addressin cell adhesion molecule-1 (MAdCAM-1) and CCL25 (TECK), respectively, which are expressed on the cell surface of endothelial cells in submucosal post-capillary venules. In the intestine, mucosal dendritic cells (DCs) in gut-associated lymphoid tissues (GALT) regulate the expression of integrin α4β7 on activated effector and regulatory lymphocytes in a retinoic acid-dependent manner [36 Iwata M, Hirakiyama A, Eshima Y, Kagechika H, Kato C, Song
SY. Retinoic acid imprints gut-homing specificity on T cells
Immunity 2004; 21: 527-38.]. Integrin α4β7+ T cells reside the lamina propria in submucosa as lamina propria lymphocytes (LPL) and can differentiate into integrin αEβ7+ T cells upon exposure to TGF-β and expression of integrin αEβ7 facilitates retention of lymphocytes in the epithelium via interactions with E-cadherin [37 Ericsson A, Svensson M, Arya A, Agace WW. CCL25/CCR9
promotes the induction and function of CD103 on intestinal
intraepithelial lymphocytes Eur J Immunol 2004; 34: 2720-9.] (Fig. 2 ). Integrin αEβ7 is a specific marker of IELs residing in mucosal epithelia and those cells expressing this antigen on their surface were initially educated in the gut.
). Integrin αEβ7 is a specific marker of IELs residing in mucosal epithelia and those cells expressing this antigen on their surface were initially educated in the gut.
Several studies have demonstrated that human genital tract mucosa expresses MAdCAM-1 endogenously [38 Trimble CL, Clark RA, Thoburn C, et al. Human Papillomavirus 16-associated cervical intraepithelial neoplasia in humans excludes CD8 T cells from dysplastic epithelium J Immunol 2010; 185: 7107-14.] and that GALT-derived integrin α4/Eβ7+ T cells home to the genital mucosa [39 Pudney J, Quayle AJ, Anderson DJ. Immunological micro-environments in the human vagina and cervix: Mediators of cellular immunity are concentrated in the cervical transformation zone Biol Reprod 2005; 73: 1253-63.-41 Kojima S, Kawana K, Fujii T, et al. Characterization of intraepithelial lymphocytes (IELs) residing in the cervical mucosa of patients with human papillomavirus (HPV)-infected intraepithelial neoplastic lesions Am J Reprod Immunol 2011; 66: 435-.]. This T cell homing and the expression of integrin αE increase in the presence of cervicitis and vaginitis [39 Pudney J, Quayle AJ, Anderson DJ. Immunological micro-environments in the human vagina and cervix: Mediators of cellular immunity are concentrated in the cervical transformation zone Biol Reprod 2005; 73: 1253-63., 40 Kelly KA, Wiley D, Wiesmeier E, Briskin M, Butch A, Darville T. The combination of the gastrointestinal integrin (α4β7) and selectin ligand enhances T-cell migration to the reproductive tract during infection with Chlamydia trachomatis Am J Reprod Immunol 2009; 61: 446-52.]. Although integrin β7+ mucosal T cells have been found in the cervical mucosa, a local inductive site (i.e., MALT) has never been demonstrated histologically [39 Pudney J, Quayle AJ, Anderson DJ. Immunological micro-environments in the human vagina and cervix: Mediators of cellular immunity are concentrated in the cervical transformation zone Biol Reprod 2005; 73: 1253-63., 40 Kelly KA, Wiley D, Wiesmeier E, Briskin M, Butch A, Darville T. The combination of the gastrointestinal integrin (α4β7) and selectin ligand enhances T-cell migration to the reproductive tract during infection with Chlamydia trachomatis Am J Reprod Immunol 2009; 61: 446-52.]. Taken together, GALT is thought to act as the inductive site for cervical IELs. GALT and the cervical mucosal connect through mucosa-specific T cells which express the homing receptors, integrin β7 and/or CCR9. Using flow cytometry, we have demonstrated that 25-30% of CD3-positive mucosal cervical lymphocytes are positive for the homing receptors integrin β7 and CCR9 and are thereby educated in GALT [41 Kojima S, Kawana K, Fujii T, et al. Characterization of intraepithelial lymphocytes (IELs) residing in the cervical mucosa of patients with human papillomavirus (HPV)-infected intraepithelial neoplastic lesions Am J Reprod Immunol 2011; 66: 435-.]. Approximately half of the integrin β7-positive T cells are CD45RO memory T cells while the other half are CD45RA effector T cells. Accumulation of integrin αEβ7+ IEL in CIN lesions varies markedly among patients and higher IEL numbers are associated with spontaneous regression of CIN [41 Kojima S, Kawana K, Fujii T, et al. Characterization of intraepithelial lymphocytes (IELs) residing in the cervical mucosa of patients with human papillomavirus (HPV)-infected intraepithelial neoplastic lesions Am J Reprod Immunol 2011; 66: 435-.]. These and related investigations have dramatically improved our understanding of cervical mucosal immunity which should hasten the development of a therapeutic HPV vaccine.
ORAL ADMINISTRATION OF HPV THERAPEUTIC VACCINES: A NOVEL APPROACH
Mucosal vaccination via oral administration of vaccine antigen is an effective method for the induction of mucosal immunity. Bermudez-Humaran et al. have evaluated the induction of CTL activity and the prevention/reduction of tumor formation following nasal or oral administration of live lactobacillus engineered to produce lactic acid-expressing HPV16E7 and IL-12, in tumor challenged murine models [42 Bermúdez-Humarán LG, Cortes-Perez NG, Lefèvre F, et al. A novel mucosal vaccine based on live Lactococci expressing E7 antigen and IL-12 induces systemic and mucosal immune responses and protects mice against human papillomavirus type 16-induced tumors J Immunol 2005; 175: 7297-302.]. They found more marked induction of mucosal responses after nasal vs oral administration and a more effective induction of immunity when using Lactobacillus plantarumvsLactococcus lactis [43 Cortes-Perez NG, Lefèvre F, Corthier G, Adel-Patient K, Langella P, Bermúdez-Humarán LG. Influence of the route of immunization and the nature of the bacterial vector on immunogenicity of mucosal vaccines based on lactic acid bacteria Vaccine 2007; 25: 6581-8.]. Poo et al. have shown that oral immunization of C57BL/6 mice with Lactobacillus casei expressing HPV16 E7 reduces tumor formation induced by TC-1 cell administration. Immunization in these experiments elicited type 1 T cell immune responses to E7 in lymphocytes isolated from the spleen and from anogenital regional lymph nodes [44 Poo H, Pyo HM, Lee TY, et al. Oral administration of human papillomavirus type 16 E7 displayed?? on Lactobacillus casei induces E7-specific antitumor effects in C57/BL6 mice Int J Cancer 2006; 119: 1702-9.]. Although both studies used transmucosal immunization with Lactobacillus-based vaccines, they examined E7-specific systemic cellular immune response and regression of subcutaneous TC-1-induced tumors. These investigations provide no insight into mucosal cellular immune responses after immunization nor into the antigen specificity of mucosal lymphocytes. We have observed a marked induction of mucosal T cells possessing HPV16 E7-specific cellular immune recognition (E7-CMI) within intestinal mucosa after oral administration of Lactobaccilus casei expressing HPV16 E7 in mice [45 Adachi K, Kawana K, Yokoyama T, et al. Oral immunization with Lactobacillus casei vaccine expressing human papillomavirus (HPV) type 16 E7 is an effective strategy to induce mucosal cytotoxic lymphocyte against HPV16 E7 Vaccine 2010; 28: 2810-7.]. In these studies, full-length mutated E7 was transduced into the Lactobacillus casei common to many lactic acid containing foods, and the bacterial cells were attenuated to the destroy exogenous plasmid gene. We compared mucosal vaccination via oral administration of the agent (GLBL101c) to systemic vaccination via intramuscular or subcutaneous injection of HPV16 E7 protein. Intramuscular and subcutaneous antigen administration induced small numbers of mucosal E7-CMI, but oral administration doubled these levels [45 Adachi K, Kawana K, Yokoyama T, et al. Oral immunization with Lactobacillus casei vaccine expressing human papillomavirus (HPV) type 16 E7 is an effective strategy to induce mucosal cytotoxic lymphocyte against HPV16 E7 Vaccine 2010; 28: 2810-7.]. This implies that oral vaccination may surmount some of the deficiencies seen with systemic immunization that have been documented in previous clinical trials. Our preclinical data encouraged us to embark on a clinical trial using GLBL101c, which has now been advanced to the Ph-I/IIa stage. Patients with CIN3 who are positive for only for HPV16 alone are presently being enrolled in dose escalation study of the effects of orally administer GLBL101c on the progression or remission of their neoplastic lesions (unpublished data).
SUMMARY
The utility of the commercially-available HPV vaccines is great but incomplete. These vaccines are a valuable step toward the control of cervical cancer and should be advanced for worldwide distribution. However, cervical cancer and its precursor lesions cannot be eradicated extant vaccination strategies costly cervical cytology screening will remain essential until new, more broadly protective HPV vaccines are developed and vaccination coverage approaches 100 % among adolescents worldwide. Until then, strategies for the development of the next generation of HPV vaccines must include both prevenative and therapeutic products.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflicts of interest.
ACKNOWLEDGEMENTS
We are grateful to Dr. Terufumi Yokoyama for excellent experiments concerning oral vaccination of GLBL101c to mice and human cervical intraepithelial lymphocytes in CIN patients and Dr. D. J. Schust for careful and critical editing of the manuscript.
REFERENCES
Endorsements
Browse Contents
Table of Contents
- EPIDEMIOLOGY OF HPV INFECTION
- NATURAL HISTORY OF CERVICAL INTRAEPITHELIAL NEOPLASIA
- SHORTCOMINGS OF THE CURRENT L1-VLP VACCINES
- DEVELOPMENT OF HPV THERAPEUTIC VACCINES
- THE CERVICAL MUCOSAL IMMUNE SYSTEM AND HPV THERAPEUTIC VACCINES
- ORAL ADMINISTRATION OF HPV THERAPEUTIC VACCINES: A NOVEL APPROACH
- SUMMARY