- Home
- About Journals
-
Information for Authors/ReviewersEditorial Policies
Publication Fee
Publication Cycle - Process Flowchart
Online Manuscript Submission and Tracking System
Publishing Ethics and Rectitude
Authorship
Author Benefits
Reviewer Guidelines
Guest Editor Guidelines
Peer Review Workflow
Quick Track Option
Copyediting Services
Bentham Open Membership
Bentham Open Advisory Board
Archiving Policies
Fabricating and Stating False Information
Post Publication Discussions and Corrections
Editorial Management
Advertise With Us
Funding Agencies
Rate List
Kudos
General FAQs
Special Fee Waivers and Discounts
- Contact
- Help
- About Us
- Search


The Open Leukemia Journal
(Discontinued)
ISSN: 1876-8164 ― Volume 5, 2013
Monitoring of Vascular Endothelial Growth Factor in POEMS Syndrome
J Minarik *, 1, V Scudla1, J Bacovsky1, T Pika1 , P Petrova2
Abstract
POEMS syndrome is a clinical unit with a very heterogenous clinical behavior. Its diagnostics as well as monitoring are not easy and depend on clinician´s experience. We present three case reports of patients with POEMS syndrome with different clinical manifestation and course of the disease. Our presentation demonstrates the benefit of the use of biochemical parameter VEGF (vascular endothelial growth factor). Retrospective analysis revealed that VEGF behaved accordingly with the state of the disease, i.e. it increased in active phase and decreased with remission of the disease. We suggest the use of VEGF not only for the diagnostics but also as a potential marker of therapeutic response and for monitoring of the course of POEMS syndrome.
Article Information
Identifiers and Pagination:
Year: 2010Volume: 3
First Page: 74
Last Page: 78
Publisher Id: TOLEUKEMIAJ-3-74
DOI: 10.2174/1876816401003010074
Article History:
Received Date: 4/6/2010Revision Received Date: 19/8/2010
Acceptance Date: 26/8/2010
Electronic publication date: 29/10/2010
Collection year: 2010
open-access license: This is an open access article licensed under the terms of the Creative Commons Attribution Non-Commercial License(http: //creativecommons.org/licenses/bync/3.0/) which permits unrestricted, non-commercial use, distribution and reproduction in any medium, provided the work is properly cited.
* Address correspondence to this author at the Department of Internal Medicine III, University Hospital Olomouc, I. P. Pavlova 6 775 20 Olomouc, Czech Republic; Tel: 420-585-3362; Fax: 420-585-2526; E-mail: abretina@email.cz
| Open Peer Review Details | |||
|---|---|---|---|
| Manuscript submitted on 4-6-2010 |
Original Manuscript | Monitoring of Vascular Endothelial Growth Factor in POEMS Syndrome | |
INTRODUCTION
POEMS syndrome (P = polyneuropathy, O = organomegaly, E = endocrinopathy, M = monoclonal gammopathy, S = skin changes) is a rare clinical unit belonging to plasma cell dyscrasias [1Dispenzieri A, Rajkumar SV, Kyle RA. Diagnosis and treatment of POEMS syndrome Treatment of multiple myeloma and related disorders 2009; 182-95.]. Unlike multiple myeloma (MM), it is usually manifested in younger patients, and its course is less aggressive [2Rajkumar SV, Kyle RA, Suarez GA, Gertz MA, Greipp PR. Neuropathy associated with plasma cell proliferative disorders.Multiple myeloma and related plasma cell disorders Mayo Foundation for medical education and research 2004; 35-52.].
The presenting symptoms include obligatory chronic progressive polyneuropathy and the presence of monoclonal immunoglobulin (almost exclusively with lambda light chain). The other characteristic features of the acronyme (organomegaly, endocrinopathy, skin changes) are variably present and sometimes difficult to unreveal, and many of the patients are treated as other (usually neurological) disorders.
The previously used diagnostic criteria were too vague and enabled the inclusion of different unrelated conditions solely on the coincidence of the symptoms [3Dispenzieri A, Kyle RA, Lacy MQ, et al. POEMS syndrome definitions and long-term outcome Blood 2003; 101: 496-506.]. The current opinion on this disease has recently changed the criteria into a more coherent panel (Table 1) [4Dispenzieri A. Mayo Clinic Criteria for the Diagnosis of Polyneuropathy, Organomegaly, Endocrinopathy, Monoclonal Gammopathy, and Skin Changes Syndrome. Note. From "POEMS Syndrome Blood Rev 2007; 21: 287.]. Interestingly, one of the major molecules which is thought to be responsible for the pathogenesis of the disease, the vascular endothelial growth factor (VEGF), is nowadays being regarded as one of the major criteria in POEMS syndrome diagnostics [5Watanabe O, Maruyama I, Arimura K, et al. Overproduction of vascular endothelial growth factor/vascular permeability factor is causative in Crow-Fukase (POEMS) syndrome Muscle Nerve 1998; 21: 1390-7.,6Dispenzieri A. POEMS Syndrome Blood Rev 2007; 21: 285-99.].
Criteria of POEMS Syndrome – Mayo Clinic Criteria from 2003 [3Dispenzieri A, Kyle RA, Lacy MQ, et al. POEMS syndrome definitions and long-term outcome Blood 2003; 101: 496-506.] and 2007 [4Dispenzieri A. Mayo Clinic Criteria for the Diagnosis of Polyneuropathy, Organomegaly, Endocrinopathy, Monoclonal Gammopathy, and Skin Changes Syndrome. Note. From "POEMS Syndrome Blood Rev 2007; 21: 287.]
We present three different manifestations of the disease with stress placed on the role of VEGF (measured by quantitative sandwich enzyme immunoassay) as an emerging diagnostic tool as well as a possible parameter of the activity of the disease.
METHODS AND RESULTS
Case Report 1
The first patient was a male, age 81, originally led under a neurological diagnosis of CIDP (Chronic Inflammatory Demyelinating Polyneuropathy) and treated using corticosteroids (Prednisone) from 9/1997. When presented at our hematology department in 10/1998, the diagnosis of POEMS was made within one week as majority of the classical symptoms were present.
The polyneuropathy was very serious with both axon and myelin damage (according to electromyography – EMG and electroneurography – ENG), the patient was unable to walk, and the activities of daily living were substantially affected. He had enlarged lymph nodes in his armpits, and the histobiopsy confirmed Castleman´s disease. The endocrinology screening revealed elevated prolactin, FSH, urine cortisol, blood glucose and C-peptide. Bone marrow biopsy confirmed slightly increased number of monoclonal lymphoplasmocytic elements (5,2%), and in both the serum and spinal fluid we found monoclonal protein IgG lambda. Within the physical examination, we saw hyperpigmentation of the chest and back, hypertrichosis, thickening of the skin and several angiomas both on the body and the limbs.
The patient presented several accompanying symptoms in the diagnostic criteria [3Dispenzieri A, Kyle RA, Lacy MQ, et al. POEMS syndrome definitions and long-term outcome Blood 2003; 101: 496-506.], such as trombocytosis (485 x109/L), the presence of osteosclerotic lesions on the X-ray of his arms, and weight loss.
The patient was treated using radiotherapy aimed at the osteosclerotic lesions of his arms, and by conventional chemotherapy (Melphalan + Prednisone). After treatment, the patient improved with the increase of muscle strength, restitution of walking, and normalization of the size of increased lymph nodes. The values of blood count and endocrine parameters normalized together with the decrease (but still persistence) of monoclonal immunoglobulin and the presence of bone marrow clonal plasma cells. The neuropathy, however, remained with no improvement.
We retrospectively analyzed plasma levels of VEGF, which were not evaluated at the time of diagnosis but sporadically within the course of the disease. Higher levels (above 2000ng/L) were found in the active phase of the disease together with worsening of accompanying symptoms, whilst in remission after treatment, the values were lower (297,0ng/L, 502,4ng/L and 824,5ng/L), only two of them reaching the normal range (62-707 ng/L).
The course of the disease had several subsequent progressions followed by remission of the disease. In 9/2008 the patient died after 11 years of the disease course of an unrelated condition (cardiac failure due to severe mitral insufficiency).
Case Report 2
A 43-years old woman with a neurological diagnosis of CIDP, was treated with Azathioprin and Prednisone (based on poor effect of steroid alone). Due to the finding of a small peak of monoclonal immunoglobulin IgG lambda (7,2g/l) she was investigated at our hematology department in 2004. She had several co-morbidities, still, the clinical investigation as well as the laboratory findings did not initially support the correct diagnosis although POEMS syndrome was one of the differentially diagnostic possibilities. The woman was obese with a long lasting type 2 diabetes without adequate compensation. The initial polyneuropathy (both sensitive and motor according to EMG) was therefore thought to be caused by CIDP and partly by diabetes, especially when there was no pathology found in the sural nerve biopsy (normal histological finding without axon loss or demyelinisation). The abdominal ultrasonography described slightly enlarged liver, probably due to steatosis, the spleen as well as lymph nodes were normal. The endocrine screening found just a mild impairment of glucose metabolism (insulin, C-peptide), associated with poorly compensated diabetes mellitus. Physical examination revealed a few benign hemangiomas of the body and the limbs. The blood count and biochemistry spectrum were normal. Bone marrow examination (including trephine biopsy) was without the presence of clonal plasmocytes and the X-ray finding was physiological. At this time the plasma cell dyscrasia was described as a monoclonal gammopathy of undetermined significance (MGUS) with no need of hematological treatment.
Within one year, however, we could see a continuous worsening of the symptoms with no effect of neurological approach and immunomodulatory therapy. Moreover, the patient had an eruption of several skin hemangiomas. We reassessed the patient with newly present anemia, focal accumulation of clonal plasma cells in the bone marrow, and with several osteolytic lesions of the skull. The conventional 99mTc scintigraphy and CT found a small locus of osteoplastic/osteosclerotic remodelation in the distal sternum. These findings supported the diagnosis of osteosclerotic myeloma, respectively POEMS syndrome.
The patient was treated with radiotherapy of the sternum and high-dosed chemotherapy followed by autologous stem cell transplantation. Chemotherapy led to a partial remission of the disease with normalization of blood count, decrease of monoclonal immunoglobulin and bone marrow plasma cell involvement, still with persistent neuropathy of the lower limbs. Therefore, after a 2-month recovery period following the transplant, we continued with conventional chemotherapy regimen (Melphalan plus Prednisone and later Cyclophosphamide plus Dexamethasone). Novel drugs (thalidomide and bortezomib) were not used for the treatment due to severe peripheral neuropathy.
With the knowledge of VEGF being suspect of the disease onset, we traced its levels in the course of the disease. The highest level, 1960,2 ng/L (normal range 62-707 ng/L) was observed at diagnosis, followed by its slow decrease corresponding to the treatment response, and an increase within the relative activation of the disease after 2-month treatment withdrawal (Fig. 1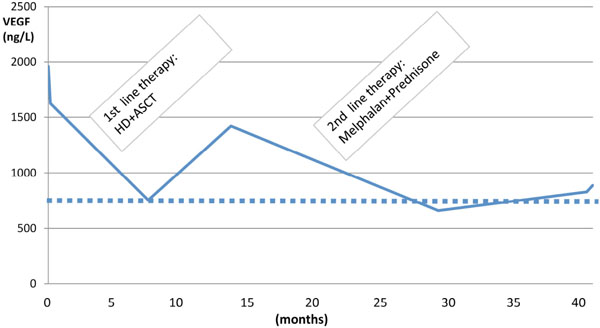 ). Within the next course, following the chemotherapy, the VEGF level decrease continued, and it finally attained the normal range.
). Within the next course, following the chemotherapy, the VEGF level decrease continued, and it finally attained the normal range.

At the moment the patient is slowly progressing with the eruption of skin hemangiomas and the increase of paraprotein. The progression is accompanied by the elevation of VEGF.
Case Report 3
A 25-year old man had an 8-month history of polyradiculoneuritis. After the initial treatment with Azathioprie and Methylprednisolone (due to poor response to Methylprednisolone alone) at the neurological department, he improved and started rehabilitiation with the interruption of immunosupressive treatment. This was complicated by the development of a severe condition with polyserositis (lower limb edema, ascites), dyspnea (pleural and cardiac effusions), and paraparesis of lower limbs. He lost 25kg in 8 months. The initial screening for possible infectious, malignant or systemic cause was negative. Except thrombocytosis 1016 x109/L and the presence of monoclonal immunoglobulin IgG lambda, there was no other impairment in laboratory findings. Repeated analyses showed normal biochemistry including CRP, total protein, albumin, creatinine, BUN. Infectious disease screening was negative, screening for onkomarkers showed no alteration, immunological screening and endocrine tests were physiological.
Except of ascites, pleural and cardiac effusions, there was no alteration in parenchymatous organs, the tests of the aspirate of both pleural effusion and ascites confirmed transsudate with no biochemical or cytological pathology. Assessment of liquor was negative and the results of bone marrow trephine biopsy including immunophenotyping were normal.
The suggestion of POEMS syndrome was supported by vast imaging findings (with no complimentary symptoms), including mixed osteolytic-osterosclerotic lesions of proximal femur, ribs, vertebral bodies and clavicles on X-ray, MRI and PET/CT. The definitive diagnosis was confirmed by the finding of compact infiltrate of monoclonal plasmocytes from the targeted biopsy of one of the larger lesions (right clavicle).
The patient was treated using radiotherapy aimed at two larger osteosclerotic lesions of left femur and right clavicle, and using high-dosed chemotherapy with preparation for autologous transplant. The stem cell harvest was, however, unsuccessful (twice in 2 month interval), with severe neutro and trombocytopenia, probably due to long-time non-specific pretreatment. The recovery period after the attempts at the harvest was followed by the reactivation of the disease. The following therapy consisted of conventional chemoterapeutics (Melphalan plus Prednisone), and led to the disappearance of effusions and improvement of overall condition including slow improvement of peripheral neuropathy, recalcification of the osteolytic lesions, normalization of blood count, and restitution of normal walking.
The plasma level of VEGF measured at the time of diagnosis was over the measurable range (more than 2000 ng/L). After diagnosis, the patient was treated with high-dosed chemotherapy, which led to a short-term stabilization of the disease and a decrease of VEGF into normal levels (505,3 ng/L). Within the course, there were two unsuccessful attempts at stem cell harvest followed by a recovery period without chemotherapy, and thus by the reactivation of the disease together with an increase of VEGF levels. Within the next course (during the chemotherapy), VEGF behaved correspondingly to the activity of the disease with a slow decrease in the normal range (Fig. 2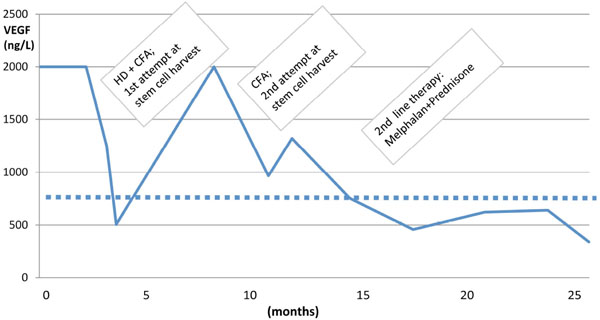 ).
).

At present, the patient is in remission with no concurrent therapy.
DISCUSSION
POEMS syndrome represents a very complex disease with variable presence of accompanying symptoms. Except for characteristic polyneuropathy and monoclonal gammopathy, the other associated symptoms might not be evident at the onset of the disease. Or, similarly as in the case report 2, they might be obscure and related to other concomitant diseases. It is therefore necessary, that the assessment is carried out by an experienced physician, and every polyneuropathy associated with monoclonal gammopathy (especially with the presence of light chain lamda) should be investigated for the signs of POEMS syndrome. Recent studies aim at the biology of the disease with the expectation of possible molecules specific for the disease.
The pathogenesis of POEMS syndrome has been intensively studied. It is supposed to be caused by the imbalance between pro-inflammatory cytokines, IL-1β, IL-6 and TNFα. The actual impulse responsible for the onset of the disease is thought to be the elevation of vascular endothelial growth factor - VEGF.
VEGF is reckoned to be responsible for majority of the symptoms. Increasing microvascular permeability leads to edema of neural tissue, increased endoneural pressure and exposure of myelin to serum cytokines which cause demyelination[7Watanabe O, Arimura K, Kitajima I, et al. Greatly raised vascular endothelial growth factor (VEGF) in POEMS syndrome Lancet 1996; 347: 702.,8Hayashi T. POEMS syndrome and VEGF Intern Med 2004; 43: 1014.].Increased vascular permeability and angiogenesis are thought to cause organomegaly, edema and skin hemangiomas,as seen in our patients[7Watanabe O, Arimura K, Kitajima I, et al. Greatly raised vascular endothelial growth factor (VEGF) in POEMS syndrome Lancet 1996; 347: 702.]. The pathogenesis, on the other hand, is more complex as the symptoms might not be present in all patients. Even our small cohort showed different manifestations from nearly physiological findings (except of peripheral neuropathy) in case report 2, to the „wet form” of POEMS syndrome with severe edema of the limbs, pleural and cardiac effusions and ascites.
VEGF is highly expressed in blood vessels and some nonmyelin forming Schwann cells [9Scarlato M, Previtali SC, Carpo M, et al. Polyneuropathy in POEMS syndrome role of angiogenic factors in the pathogenesis Brain 2005; 128: 1911-20.]. One of the major sources are thought to be the platelets [10Hashiguchi T, Arimura K, Matsumuro K, et al. Highly concentrated vascular endothelial growth factor in platelets in Crow Fukase syndrome Muscle Nerve 2000; 23: 1051-6.]. This idea is in accordance with increased levels of thrombocytes in majority of patients, and thrombocytopenia might be the reason for the lack of VEGF elevation in some patients [11Kuwabara S. Relapse of POEMS syndrome without increased level of VEGF Neuromuscular Disord 2009; 19: 740-1.]. On the other hand, even patients with low platelet count present elevated VEGF levels. The possible other sources of VEGF are osteosclerotic lesions, plasma cells, tumor cells and endothelial cells [12Nakajima H, Ishida S, Furutama D, et al. Expression of vascular endothelial growth factor by plasma cells in the sclerotic bone lesions of a patient with POEMS syndrome J Neurol 2007; 254: 531-3.,13Nobile-Orazio E, Terenghi F, Giannotta C, et al. Serum VEGF levels in POEMS syndrome and immune mediated neuropathies Neurology 2009; 72: 1024-6.].
The levels of VEGF in POEMS syndrome are usually higher than in patients with other plasma cell dyscrasias such as MGUS and multiple myeloma [1Dispenzieri A, Rajkumar SV, Kyle RA. Diagnosis and treatment of POEMS syndrome Treatment of multiple myeloma and related disorders 2009; 182-95.,14Soubrier M, Dubost JJ, Serre AF, et al. Growth factors in POEMS syndrome: evidence for a marked increase in circulating vascular endothelial growth factor Arhritis Rheum 1997; 40: 786-.,15Gherardi RK, Belec L, Soubrier M, et al. Overproduction of proinflammatory cytokines imbalanced by their antagonists in POEMS syndrome Blood 1996; 87: 1458-65.]. On the other hand, they might be affected by other conditions, such as the presence of solid tumor, inflammation, estrogen levels, hepatic disorders or even some reparative physiological processes, which make VEGF less specific for differential diagnosis. The complicated role of VEGF in the pathogenesis of POEMS syndrome has been underlined by several reports on the treatment of the disease using an anti-VEGF antibody, bevacizumab [16Badros A, Porter N, Zimrin A. Bevacizumab therapy for POEMS syndrome Blood 2005; 106: 1135.-18Samaras P, Bauer S, Stenner-Liewen F, et al. Treatment of POEMS syndrome with bevacizumab Haematologica 2007; 92: 1438-9.]. In the study of Badros et al., a patient with POEMS syndrome was sucessfully treated with bevacizumab with the decrease of VEGF, resolution of edema and vanishing of the neuropathy pain [16Badros A, Porter N, Zimrin A. Bevacizumab therapy for POEMS syndrome Blood 2005; 106: 1135.]. Contrary to this experience, in the report of Strasume et al. and Samaras et al., the patients after short-term improvement developed refractory edema and died, suggesting the impact of increased apoptosis of motor neurons and endothelial cells due to rapid decrease of VEGF [17Straume O, Bergheim J, Ernst P. Bevacizumab therapy for POEMS syndrome Blood 2006; 107: 4972-3.,18Samaras P, Bauer S, Stenner-Liewen F, et al. Treatment of POEMS syndrome with bevacizumab Haematologica 2007; 92: 1438-9.]. Nevertheless, the investigation of VEGF in POEMS syndrome has a great potential to unreveal the actual causes of the disease and to choose the optimal treatment target.
Evaluation of the course of POEMS syndrome is often very not easy and dependent on subjective assessment of the physician. There are no standard means of remission or progression of the disease, and even the values of paraprotein might not be always helpful. Remission and/or progression are therefore usually defined as the normalization or re-appearance of clinical symptoms (edema, skin lesions, lymph nodes, worsening of neuropathy) together with laboratory abnormalities (endocrine spectrum, hemoglobin levels, etc.). Our findings suggest VEGF as an emerging tool for routine assessment of the course of POEMS syndrome. There have not been many studies monitoring VEGF in the course of the disease. Kuwabara reported the normalization of VEGF levels in 4 patients with POEMS syndrome treated by autologous stem cell transplantation [19Kuwabara S, Misawa S, Kanai K, et al. Autologous peripheral blood stem cell transplantation for POEMS syndrome Neurology 2006; 66: 105-7.], some other authors described recently case reports with sequential VEGF monitoring [20Mineta M, Hatori M, Sano H, et al. Recurrent Crow–Fukase syndrome associated with increased serum levels of vascular endothelial growth factor: a case report and review of the literature Tohoku J Exp Med 2006; 210: 269-77.-22Imai N, Taguchi J, Nobuyasu Y, et al. Relapse of polyneuropathy, organomegaly, endocrinopathy, M-protein, and skin changes (POEMS syndrome) without increased level of vascular endothelial growth factor following successful autologous peripheral blood stem cell transplantation Neuromuscul Disord 2009; 19: 363-5.], still, there has not been a larger cohort study which would confirm the presented findings.
We acknowledge the limitations in the retrospective analysis, and the small number of patients precludes statistical analysis. The levels of VEGF were not evaluated in standardized intervals, and the time between drawing of the sample and the analysis of VEGF levels differed. All of the samples were first frozen and then analyzed together, usually in 2-3 month interval so the degradation as well as other external influences might have affected the final result. Studies with longer follow-up and larger number of patients will be needed to determine whether the role of VEGF in POEMS syndrome maintains only its diagnostic value or might have the potential to predict the course of the disease and become the marker of the stability and/or the activity of the disease.
CONCLUSION
Our paper contributes to the assessment of POEMS syndrome by the suggestion of longitudinal monitoring of VEGF levels in the course of the disease. The levels of VEGF behaved in accord with the activity of the disease and predicted the course of the disease better than the evaluation of paraprotein and subjective symptoms. If confirmed by larger studies, VEGF has the potential to become a pivotal marker of the disease activity and a predictor of its behavior or, at least as a surrogate marker of successful treatment of this rare disease.
The study was supported by the grant MZ CR NR 9489-3.